

Health and economic impact of HPV 16/18 vaccination and cervical cancer screening in Eastern Africa
- PMID: 21717458
- PMCID: PMC3314721
- DOI: 10.1002/ijc.26269
Health and economic impact of HPV 16/18 vaccination and cervical cancer screening in Eastern Africa
Abstract
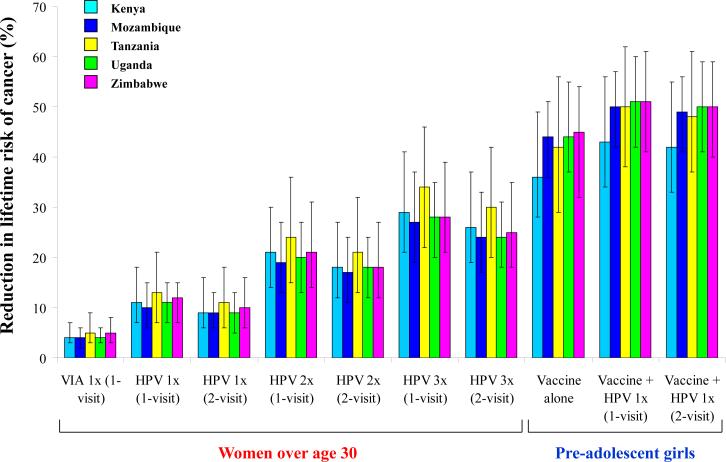
Eastern Africa has the world's highest cervical cancer incidence and mortality rates. We used epidemiologic data from Kenya, Mozambique, Tanzania, Uganda, and Zimbabwe to develop models of HPV-related infection and disease. For each country, we assessed HPV vaccination of girls before age 12 followed by screening with HPV DNA testing once, twice, or three times per lifetime (at ages 35, 40, 45). For women over age 30, we assessed only screening (with HPV DNA testing up to three times per lifetime or VIA at age 35). Assuming no waning immunity, mean reduction in lifetime cancer risk associated with vaccination ranged from 36 to 45%, and vaccination followed by screening once per lifetime at age 35 with HPV DNA testing ranged from 43 to 51%. For both younger and older women, the most effective screening strategy was HPV DNA testing three times per lifetime. Provided the cost per vaccinated girl was less than I$10 (I$2 per dose), vaccination had an incremental cost-effectiveness ratio [I$ (international dollars)/year of life saved (YLS)] less than the country-specific per capita GDP, a commonly cited heuristic for "very cost-effective" interventions. If the cost per vaccinated girl was between I$10 (I$2 per dose) and I$25 (I$5 per dose), vaccination followed by HPV DNA testing would save the most lives and would be considered good value for public health dollars. These results should be used to catalyze design and evaluation of HPV vaccine delivery and screening programs, and contribute to a dialogue on financing HPV vaccination in poor countries.
Copyright © 2011 UICC.
Figures


References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008, Cancer incidence and mortality worldwide: IARC CancerBase No. 10. International Agency for Research on Cancer; Lyon, France: 2010. [September 22, 2010]. Available online at http://globocan.iarc.fr.
-
- Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, Winer R, Clifford GM. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer. 2007;121:621–32. - PubMed
-
- World Health Organization (WHO)/Institute Català d'Oncologia (ICO) Information Centre on HPV and Cervical Cancer (HPV Information Centre) [September 22, 2010];Summary report on HPV and cervical cancer statistics in Africa. 2010 Available online at www.who.int/hpvcentre.
-
- Denny L, Quinn M, Sankaranarayanan R. Chapter 8: Screening for cervical cancer in developing countries. Vaccine. 2006;24:S71–7. - PubMed
