

Impaired fasting glucose and the risk of incident diabetes mellitus and cardiovascular events in an adult population: MESA (Multi-Ethnic Study of Atherosclerosis)
- PMID: 21718910
- PMCID: PMC3146297
- DOI: 10.1016/j.jacc.2011.03.025
Impaired fasting glucose and the risk of incident diabetes mellitus and cardiovascular events in an adult population: MESA (Multi-Ethnic Study of Atherosclerosis)
Abstract
Objectives: The purpose of the study was to assess the cardiovascular risk of impaired fasting glucose (IFG).
Background: The associations between IFG, incident type 2 diabetes mellitus (T2DM), and cardiovascular (CV) events remains unclear.
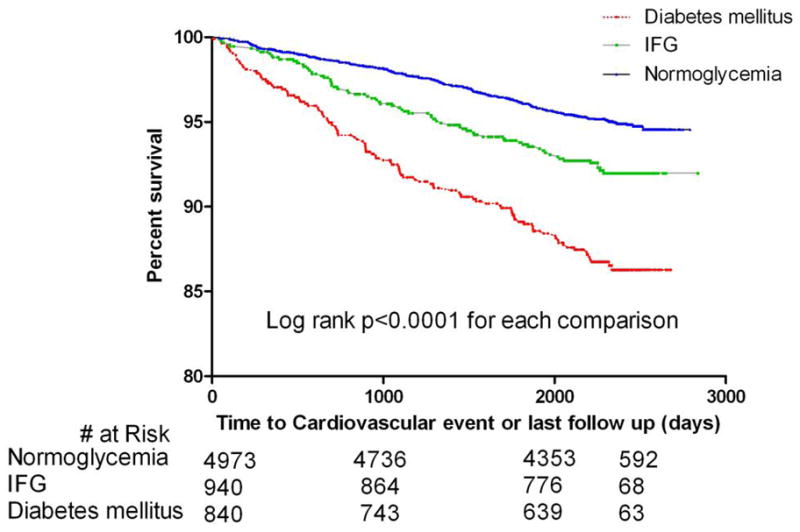
Methods: The MESA (Multi-Ethnic Study of Atherosclerosis) study included participants who were 45 to 84 years or age and free of clinical CV disease at baseline (2000 to 2002). Type 2 DM was defined as fasting glucose >125 mg/dl or receiving antidiabetes medication at baseline and follow-up examinations; IFG was defined as no T2DM and fasting glucose 100 to 125 mg/dl. Cox proportional hazards analysis was used to assess the association between IFG and incident DM and also between IFG and incident CV events.
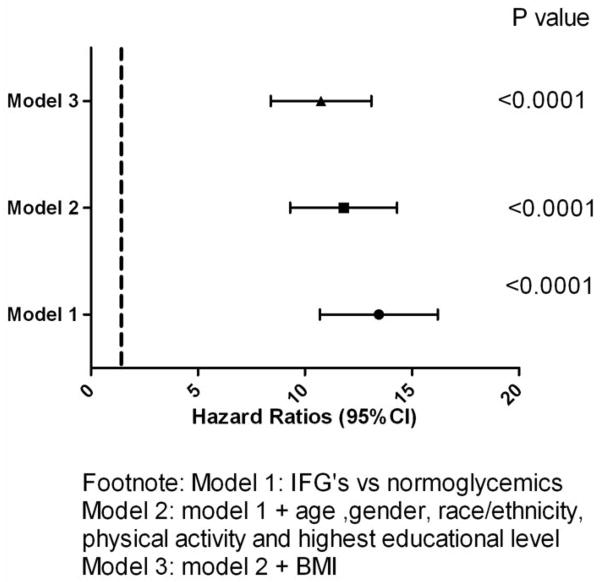
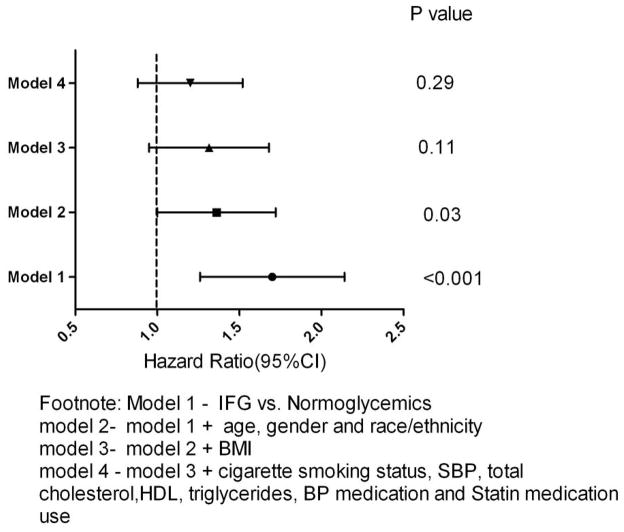
Results: Of 6,753 participants included in these analyses, 840 (12.7%) had T2DM and 940 (13.8%) had IFG at the baseline examination. During 7.5 years of follow-up, there were 418 adjudicated CV events. Type 2 DM was associated with an increased CV incidence in the univariate model (hazard ratio [HR]: 2.83, 95% confidence interval [CI]: 2.25 to 3.56, p < 0.0001) and multivariate model adjusted for demographics and traditional risk factors (HR: 1.87, 95% CI: 1.47 to 2.37, p < 0.0001) compared with subjects not having T2DM (IFG plus normal fasting glucose). Impaired fasting glucose was associated with increased incidence of T2DM (HR: 13.2, 95% CI: 10.8 to 16.2, p < 0.001) that remained after adjusting for demographics, highest educational level, physical activity, and body mass index (HR: 10.5, 95% CI: 8.4 to 13.1, p < 0.001) compared with normal fasting glucose. Impaired fasting glucose was associated with incident CV events in the univariate model (HR: 1.64, 95% CI: 1.26 to 2.14, p < 0.001) but not in the full multivariate model (HR: 1.16, 95% CI: 0.88 to 1.52, p = 0.3) compared with normal fasting glucose.
Conclusions: Having IFG was not independently associated with an increased short-term risk for incident CV events. These data reiterate the importance of intervention for persons with IFG to reduce their incidence of T2DM.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Impaired fasting glucose and the risk of incident diabetes mellitus and cardiovascular events.J Am Coll Cardiol. 2011 Dec 6;58(24):2546-7; author reply 2547. doi: 10.1016/j.jacc.2011.07.049. J Am Coll Cardiol. 2011. PMID: 22133860 No abstract available.
References
-
- Prevalence of diabetes and impaired fasting glucose in adults—United States, 1999–2000. MMWR Morb Mortal Wkly Rep. 2003;52:833–7. - PubMed
-
- Davidson MB, Landsman PB, Alexander CM. Lowering the criterion for impaired fasting glucose will not provide clinical benefit. Diabetes Care. 2003;26:3329–30. - PubMed
-
- Unwin N, Shaw J, Zimmet P, Alberti KG. Impaired glucose tolerance and impaired fasting glycaemia: the current status on definition and intervention. Diabet Med. 2002;19:708–23. - PubMed
-
- de Vegt F, Dekker JM, Jager A, et al. Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population: The Hoorn Study. JAMA. 2001;285:2109–13. - PubMed
-
- Fisman EZ, Motro M, Tenenbaum A, Boyko V, Mandelzweig L, Behar S. Impaired fasting glucose concentrations in nondiabetic patients with ischemic heart disease: a marker for a worse prognosis. Am Heart J. 2001;141:485–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- T32 HL076132/HL/NHLBI NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
