

Intrahepatic type II gall bladder perforation by a gall stone in a CAPD patient
- PMID: 21719394
- PMCID: PMC3352193
- DOI: 10.1186/2047-783x-16-5-213
Intrahepatic type II gall bladder perforation by a gall stone in a CAPD patient
Abstract
Introduction: Perforation of the gall bladder represents a rare, but life-threatening complication of cholecystitis. Clinical presentation may vary between severe peritonism in acute perforation and absence of symptoms in subacute or chronic progression of perforation. Abdominal imaging like ultrasound or CT-scan are important tools for immediate diagnose of gall bladder perforation.
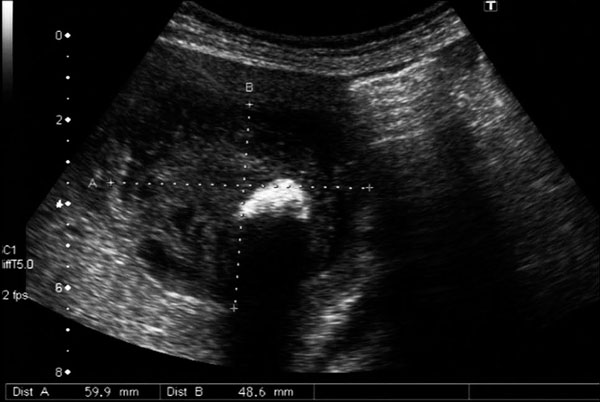
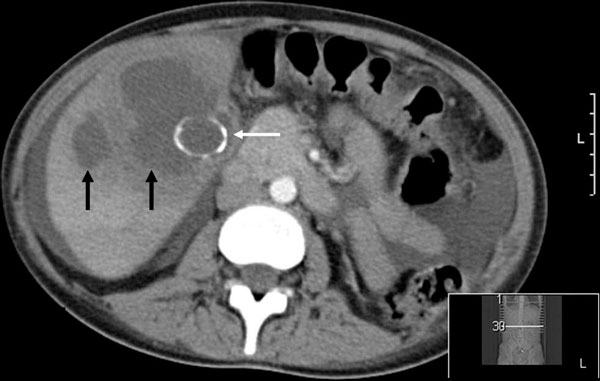
Case presentation: We report a case of a 30-year old female patient with end-stage kidney disease treated by continuous ambulatory peritoneal dialysis (CAPD) who was admitted to the emergency room with fever and mild abdominal pain. A type II gall bladder perforation by a solitary gall stone with development of a liver abscess was detected by abdominal ultrasound.
Conclusion: Gall bladder perforations are rare but have to be considered in patients with abdominal pain and fever. Abdominal ultrasound is a reliable tool to establish diagnosis.
Figures



References
-
- Wallace R, Allen A. Acute cholecystitis. Arch Surg. 1943;43(5):762–72.
-
- Larmi TK, Kairaluoma MI, Junila J, Laitinen S, Stahlberg M, Fock HG. Perforation of the gallbladder. A retrospective comparative study of cases from 1946-1956 and 1969-1980. Acta Chir Scand. 1984;150(7):557–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
