

The National Emphysema Treatment Trial (NETT) Part II: Lessons learned about lung volume reduction surgery
- PMID: 21719757
- PMCID: PMC3208657
- DOI: 10.1164/rccm.201103-0455CI
The National Emphysema Treatment Trial (NETT) Part II: Lessons learned about lung volume reduction surgery
Abstract
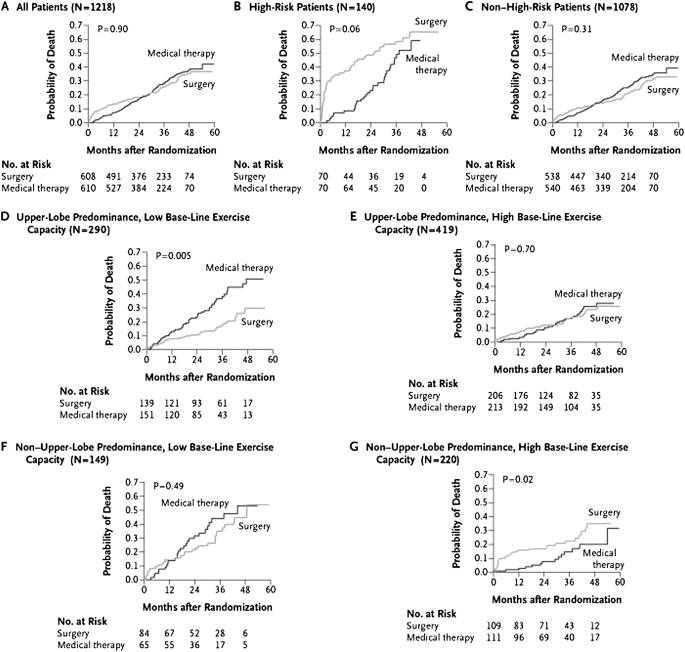
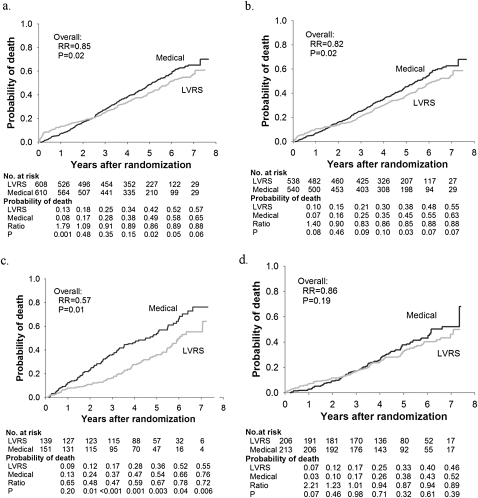
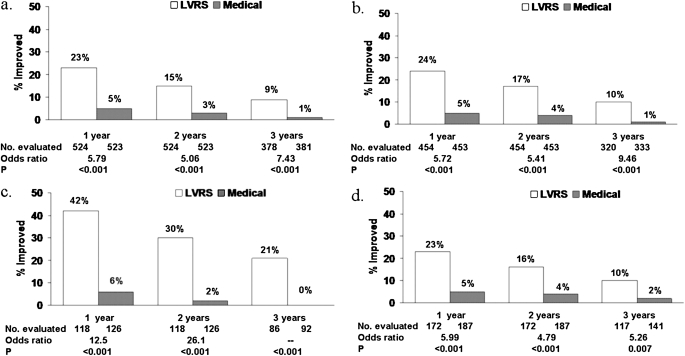
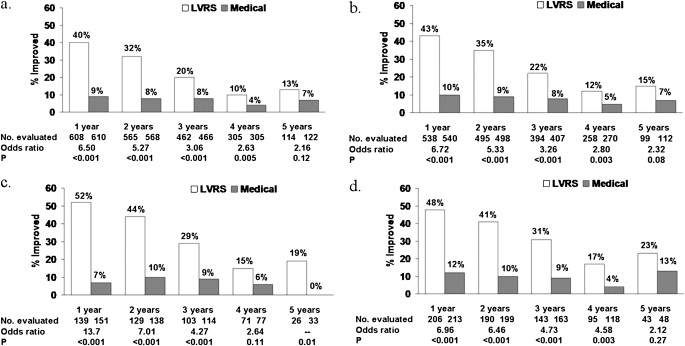
Substantial information regarding the role of lung volume reduction surgery (LVRS) in severe emphysema emanates from the National Emphysema Treatment Trial (NETT). The NETT was not a crossover trial and therefore was able to examine the effects of optimal medical management and LVRS on short- and long-term survival,as well as lung function, exercise performance, and quality of life.The NETT generated multiple insights into the preoperative, perioperative,and postoperative management of patients undergoing thoracotomy; described pain control techniques that were safe and effective; and emphasized the need to address nonpulmonary issues to optimize surgical outcomes. After the NETT, newer investigation has focused on bronchoscopic endobronchial interventions and other techniques less invasive than LVRS to achieve lung reduction.In this review, we summarize what we currently know about the role of LVRS in the treatment of severe emphysema as a result of insights gained from the NETT and provide a brief review of the newer techniques of lung volume reduction.
Figures
References
-
- Sciurba FC, Ernst A, Herth FJ, Strange C, Criner GJ, Marquette CH, Kovitz KL, Chiacchierini RP, Goldin J, McLennan G, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010;363:1233–1244 - PubMed
-
- Mineo D, Ambrogi V, Cufari ME, Gambardella S, Pignotti L, Pompeo E, Mineo TC. Variations of inflammatory mediators and α1-antitrypsin levels after lung volume reduction surgery for emphysema. Am J Respir Crit Care Med 2010;181:806–814 - PubMed
-
- Watz H, Waschki B, Meyer T, Kretschmar G, Kirsten A, Claussen M, Magnussen H. Decreasing cardiac chamber sizes and associated heart dysfunction in COPD: role of hyperinflation. Chest 2010;138:32–38 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
