

Correlation of inpatient and outpatient measures of stroke care quality within veterans health administration hospitals
- PMID: 21719771
- PMCID: PMC3144276
- DOI: 10.1161/STROKEAHA.110.611913
Correlation of inpatient and outpatient measures of stroke care quality within veterans health administration hospitals
Abstract
Background and purpose: Quality of care delivered in the inpatient and ambulatory settings may be correlated within an integrated health system such as the Veterans Health Administration. We examined the correlation between stroke care quality at hospital discharge and within 6 months postdischarge.
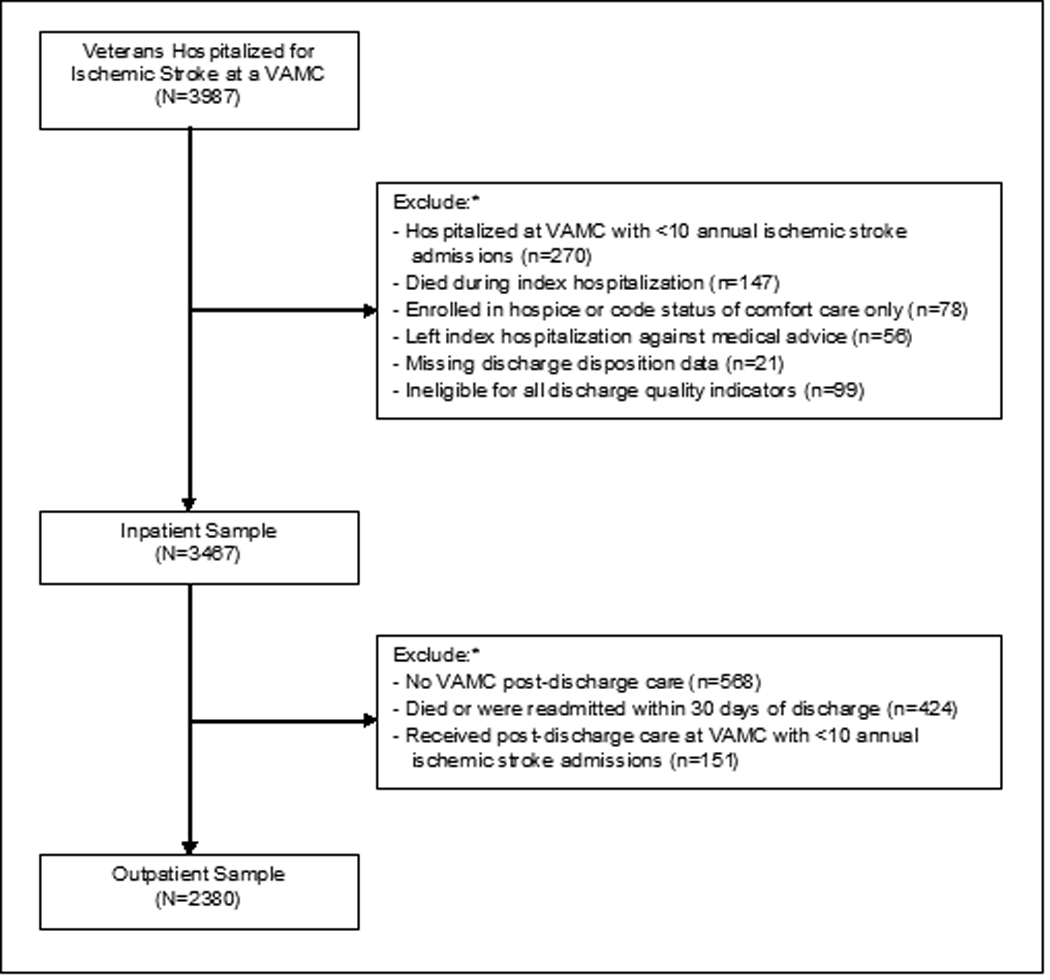
Methods: We conducted a cross-sectional hospital-level correlation analyses of chart-abstracted data for 3467 veterans discharged alive after an acute ischemic stroke from 108 Veterans Health Administration medical centers and 2380 veterans with postdischarge follow-up within 6 months in fiscal year 2007. Four risk-standardized processes of care represented discharge care quality: prescription of antithrombotic and antilipidmic therapy, anticoagulation for atrial fibrillation, and tobacco cessation counseling along with a composite measure of defect-free care. Five risk-standardized intermediate outcomes represented postdischarge care quality: achievement of blood pressure, low-density lipoprotein, international normalized ratio, and glycosylated hemoglobin target levels, and delivery of appropriate treatment for poststroke depression along with a composite measure of achieved outcomes.
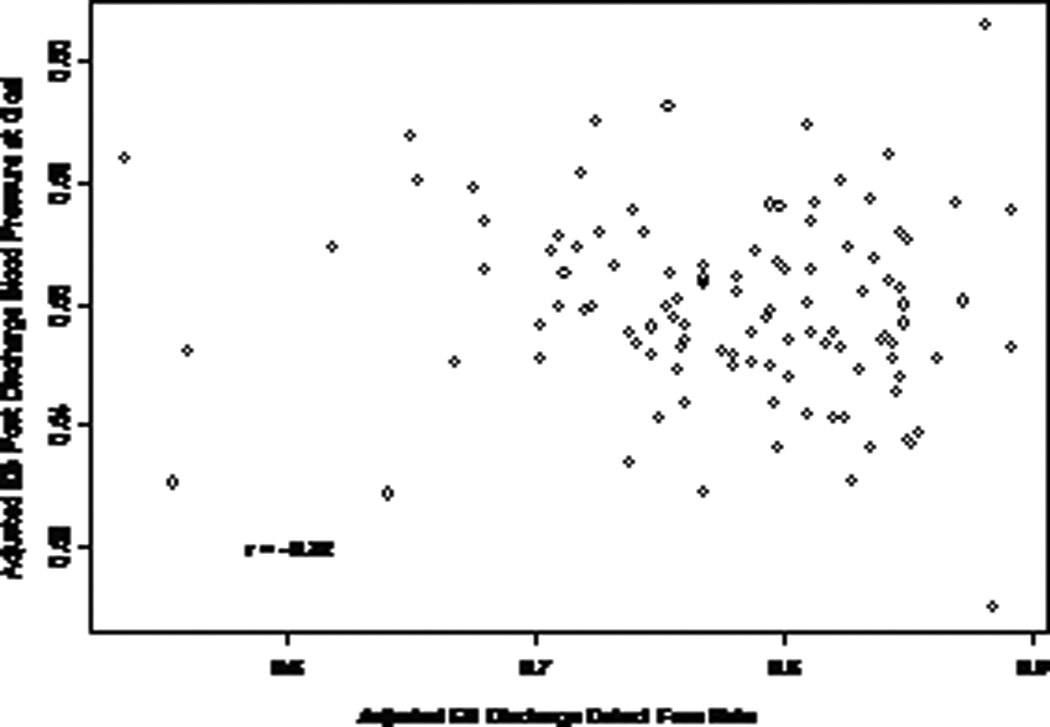
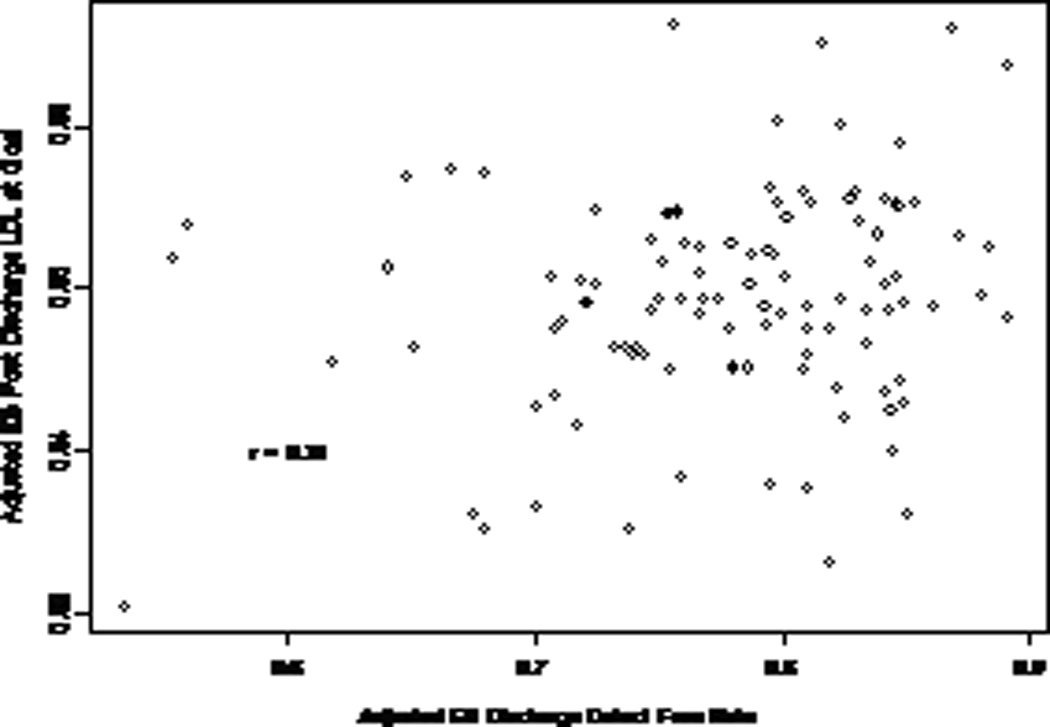
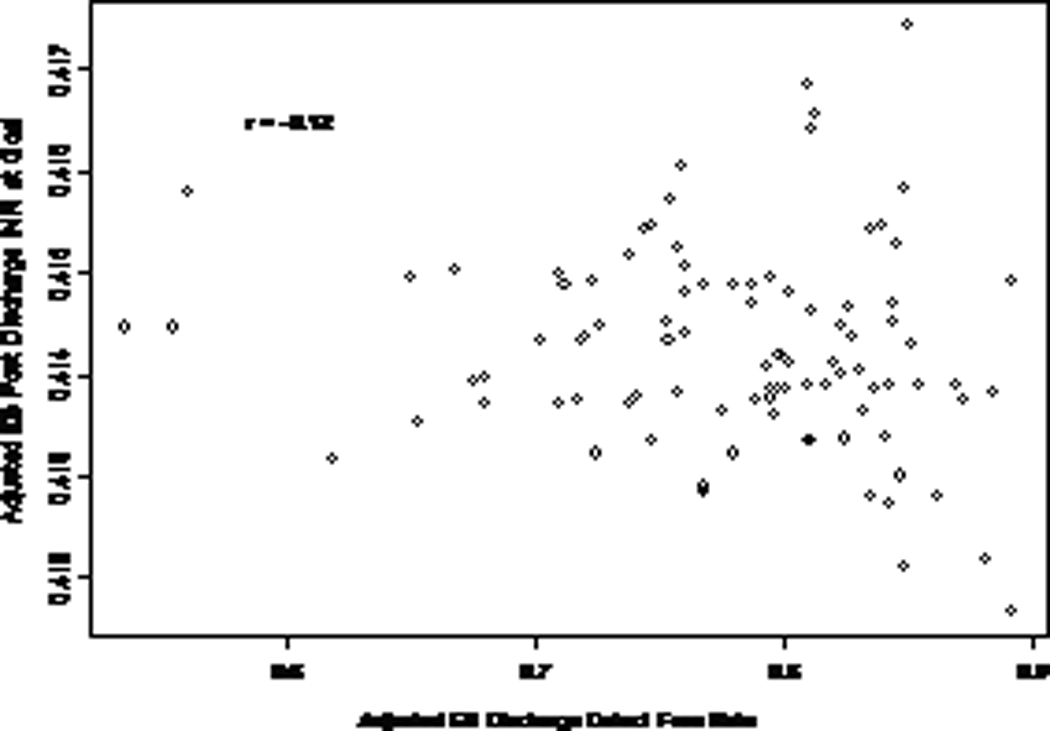
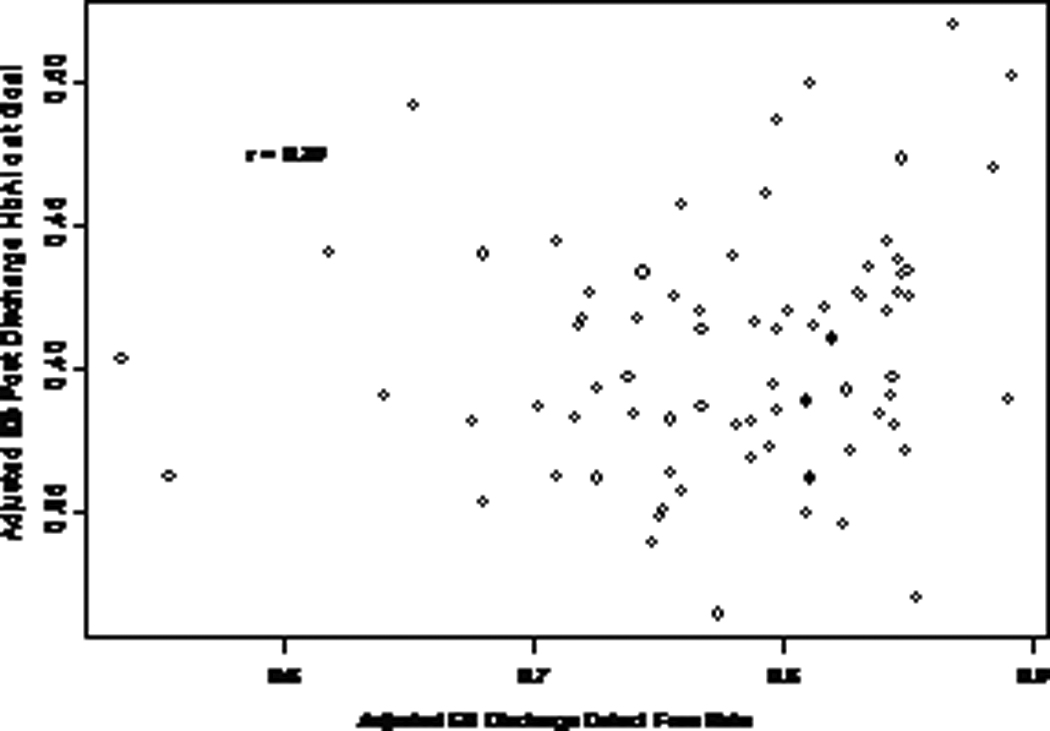
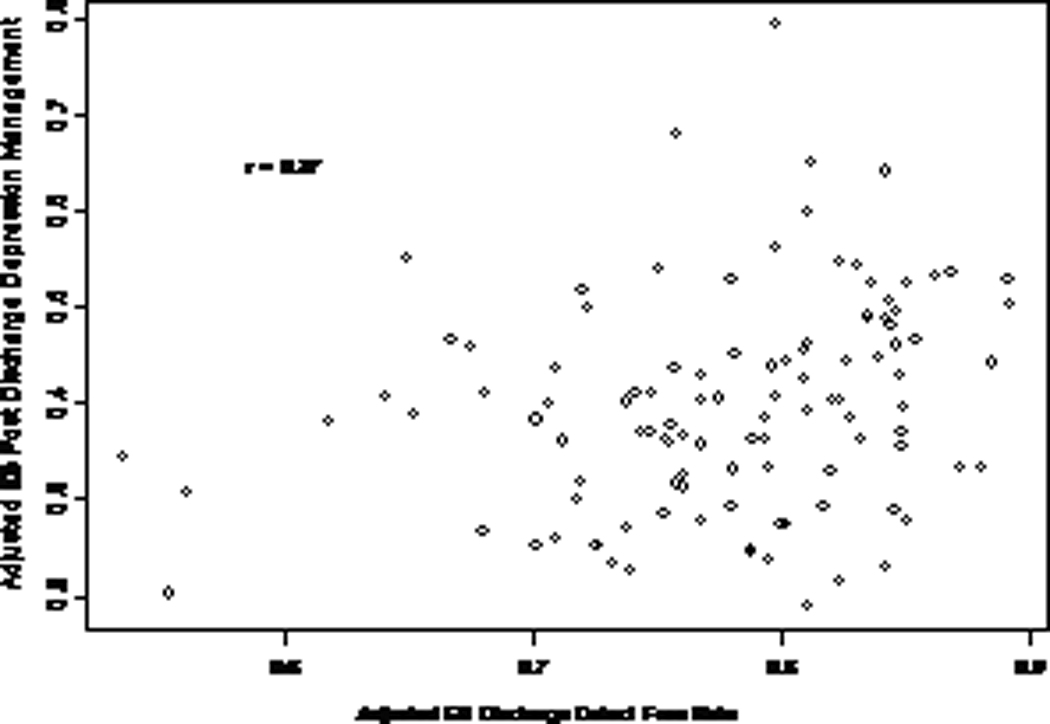
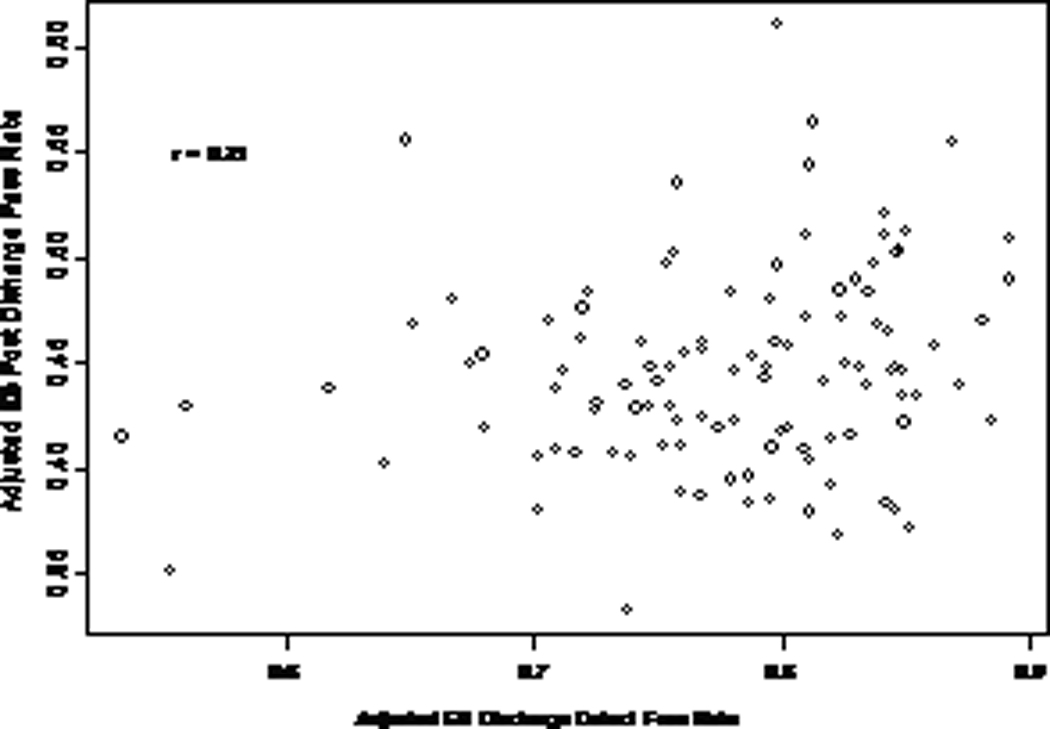
Results: Median risk-standardized composite rate of defect-free care at discharge was 79%. Median risk-standardized postdischarge rates of achieving goal were 56% for blood pressure, 36% for low-density lipoprotein, 41% for international normalized ratio, 40% for glycosylated hemoglobin, and 39% for depression management and the median risk-standardized composite 6-month outcome rate was 44%. The hospital composite rate of defect-free care at discharge was correlated with meeting the low-density lipoprotein goal (r=0.31; P=0.007) and depression management (r=0.27; P=0.03) goal but was not correlated with blood pressure, international normalized ratio, glycosylated hemoglobin goals, nor with the composite measure of achieved postdischarge outcomes (probability values >0.13).
Conclusions: Hospital discharge care quality was not consistently correlated with ambulatory care quality.
Conflict of interest statement
No financial conflicts of interest to disclose.
Figures
References
-
- Institute of Medicine. To err is human: Building a safer health system. Washington, DC: National Academy Press; 2000.
-
- Institute of Medicine. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press; 2001. - PubMed
-
- Bradley EH, Herrin J, Elbel B, McNamara RL, Magid DJ, Nallamothu BK, Wang Y, Normand SL, Spertus JA, Krumholz HM. Hospital quality for acute myocardial infarction: Correlation among process measures and relationship with short-term mortality. JAMA. 2006;296:72–78. - PubMed
-
- Peterson ED, Roe MT, Mulgund J, DeLong ER, Lytle BL, Brindis RG, Smith SC, Jr, Pollack CV, Jr, Newby LK, Harrington RA, Gibler WB, Ohman EM. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA. 2006;295:1912–1920. - PubMed
-
- Werner RM, Bradlow ET. Relationship between medicare's hospital compare performance measures and mortality rates. JAMA. 2006;296:2694–2702. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
