

Optimal end points for acute stroke therapy trials: best ways to measure treatment effects of drugs and devices
- PMID: 21719772
- PMCID: PMC3463240
- DOI: 10.1161/STROKEAHA.111.619122
Optimal end points for acute stroke therapy trials: best ways to measure treatment effects of drugs and devices
Erratum in
- Stroke. 2011 Nov;42(11):e634
Abstract
Background and purpose: Over the past decade, analysis of completed actual trials, model population studies, and theoretical work have improved approaches to selecting and analyzing end points in acute stroke treatment trials.
Methods: Narrative review.
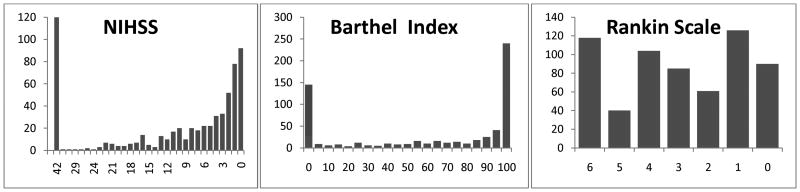
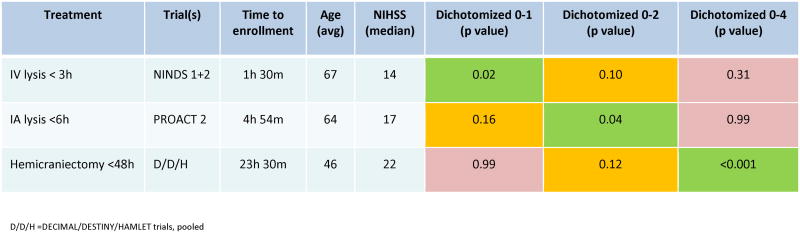
Results: Because stroke affects persons in their biological, functional, social, and experiential dimensions, measures of impairment, disability, handicap, and quality of life are all desirable in pivotal trials, with disability being most important. Scales that are valid, reliable, responsive, and easy to administer are preferred; consequently, the modified Rankin Scale has become the most widely used single clinical efficacy measure. Because stroke cripples and kills, most outcome scales array patient outcome in ordered ranks, spread over the entire range from normal to disabled to dead. Generally, shift analysis, analyzing all health state transitions concurrently, is the most efficient analytic technique to detect treatment effects, with sliding dichotomy less efficient and fixed dichotomy least efficient, unless treatment effects strongly cluster at 1 or a few health state transitions that can be prespecified. Test statistics must also take into account interpretability, ie, how well they can be converted into metrics capturing all outcomes the intervention might alter in proportion to the degree they are valued by the patient; full ordinal analysis is most informative, sliding dichotomy is intermediately informative, and fixed dichotomy is least informative regarding this global outcome.
Conclusions: Stroke trial power and interpretation can be substantially enhanced by adherence to the principles delineated in this review. Full ordinal and sliding dichotomy analysis will most often be advantageous compared with fixed dichotomous approaches.
Figures
References
-
- Hong KS, Lee SJ, Hao Q, Liebeskind DS, Saver JL. Acute stroke trials in the 1st decade of the 21th century. Stroke. 2011;42:e314.
-
- Fisher M, Albers GW, Donnan GA, Furlan AJ, Grotta JC, Kidwell CS, et al. Enhancing the development and approval of acute stroke therapies: Stroke Therapy Academic Industry Roundtable. Stroke. 2005;36:1808–13. - PubMed
-
- Higashida RT, Furlan AJ, Roberts H, Tomsick T, Connors B, Barr J, et al. Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke. 2003;34:e109–37. - PubMed
-
- Optimising Analysis of Stroke Trials Collaboration. Calculation of sample size for stroke trials assessing functional outcome: comparison of binary and ordinal approaches. Int J Stroke. 2008;3:78–84. - PubMed
-
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007;38:967–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
