

Dual manganese-enhanced and delayed gadolinium-enhanced MRI detects myocardial border zone injury in a pig ischemia-reperfusion model
- PMID: 21719779
- PMCID: PMC3178667
- DOI: 10.1161/CIRCIMAGING.110.960591
Dual manganese-enhanced and delayed gadolinium-enhanced MRI detects myocardial border zone injury in a pig ischemia-reperfusion model
Abstract
Background: Gadolinium (Gd)-based delayed-enhancement MRI (DEMRI) identifies nonviable myocardium but is nonspecific and may overestimate nonviable territory. Manganese (Mn(2+))-enhanced MRI (MEMRI) denotes specific Mn(2+) uptake into viable cardiomyocytes. We performed a dual-contrast myocardial assessment in a porcine ischemia-reperfusion (IR) model to test the hypothesis that combined DEMRI and MEMRI identifies viable infarct border zone (BZ) myocardium in vivo.
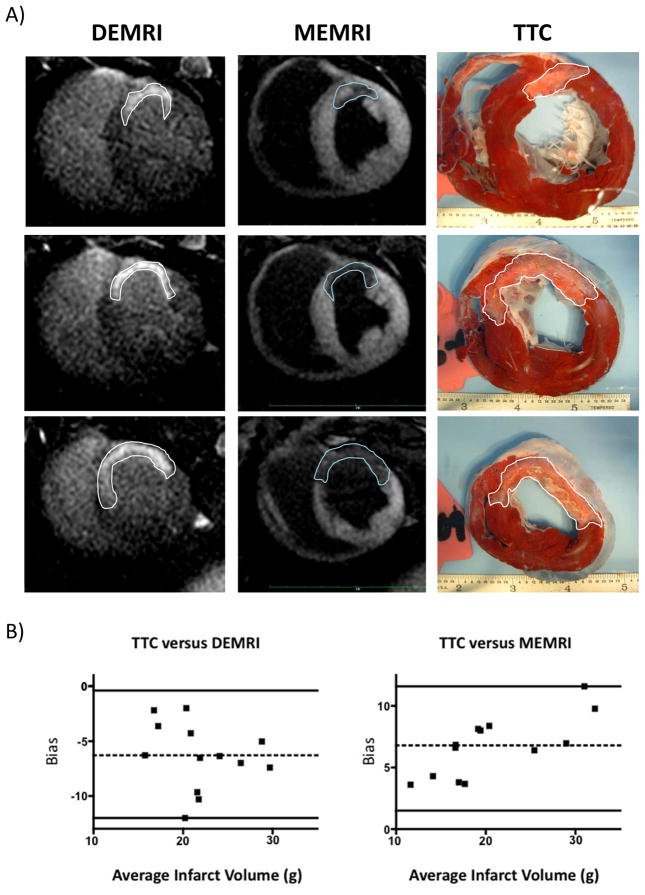
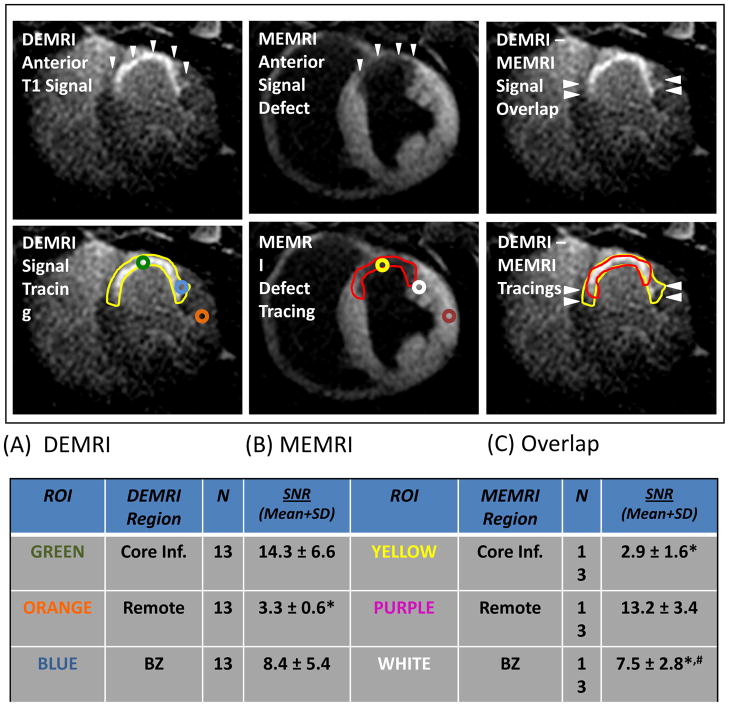
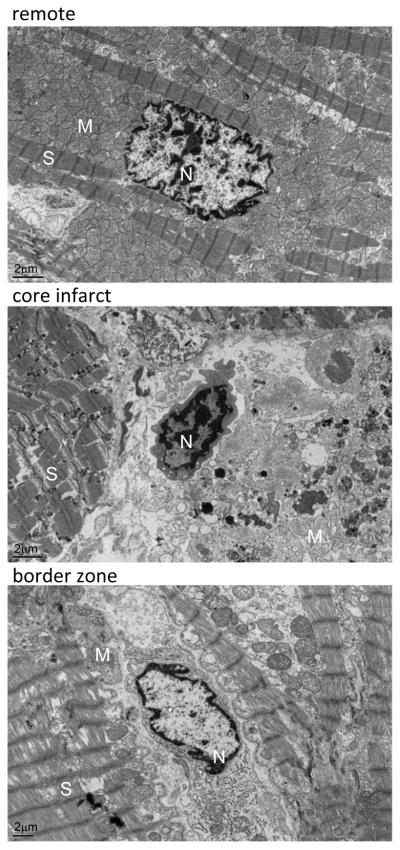
Methods and results: Sixty-minute left anterior descending coronary artery IR injury was induced in 13 adult swine. Twenty-one days post-IR, 3-T cardiac MRI was performed. MEMRI was obtained after injection of 0.7 mL/kg Mn(2+) contrast agent. DEMRI was then acquired after injection of 0.2 mmol/kg Gd. Left ventricular (LV) mass, infarct, and function were analyzed. Subtraction of MEMRI defect from DEMRI signal identified injured BZ myocardium. Explanted hearts were analyzed by 2,3,5-triphenyltetrazolium chloride stain and tissue electron microscopy to compare infarct, BZ, and remote myocardium. Average LV ejection fraction was reduced (30±7%). MEMRI and DEMRI infarct volumes correlated with 2,3,5-triphenyltetrazolium chloride stain analysis (MEMRI, r=0.78; DEMRI, r=0.75; P<0.004). MEMRI infarct volume percentage was significantly lower than that of DEMRI (14±4% versus 23±4%; P<0.05). BZ MEMRI signal-to-noise ratio (SNR) was intermediate to remote and core infarct SNR (7.5±2.8 versus 13.2±3.4 and 2.9±1.6; P<0.0001), and DEMRI BZ SNR tended to be intermediate to remote and core infarct SNR (8.4±5.4 versus 3.3±0.6 and 14.3±6.6; P>0.05). Tissue electron microscopy analysis exhibited preserved cell structure in BZ cardiomyocytes despite transmural DEMRI enhancement.
Conclusions: The dual-contrast MEMRI-DEMRI detects BZ viability within DEMRI infarct zones. This approach may identify injured, at-risk myocardium in ischemic cardiomyopathy.
Figures
Similar articles
-
Telmisartan in the diabetic murine model of acute myocardial infarction: dual contrast manganese-enhanced and delayed enhancement MRI evaluation of the peri-infarct region.Cardiovasc Diabetol. 2016 Feb 5;15:24. doi: 10.1186/s12933-016-0348-y. Cardiovasc Diabetol. 2016. PMID: 26846539 Free PMC article.
-
Myocardial viability of the peri-infarct region measured by T1 mapping post manganese-enhanced MRI correlates with LV dysfunction.Int J Cardiol. 2019 Apr 15;281:8-14. doi: 10.1016/j.ijcard.2019.01.101. Epub 2019 Jan 31. Int J Cardiol. 2019. PMID: 30739802 Free PMC article.
-
Manganese-Enhanced T1 Mapping in the Myocardium of Normal and Infarcted Hearts.Contrast Media Mol Imaging. 2018 Oct 25;2018:9641527. doi: 10.1155/2018/9641527. eCollection 2018. Contrast Media Mol Imaging. 2018. PMID: 30498403 Free PMC article.
-
Manganese-enhanced MRI of the myocardium.Heart. 2019 Nov;105(22):1695-1700. doi: 10.1136/heartjnl-2019-315227. Epub 2019 Jul 23. Heart. 2019. PMID: 31337670 Free PMC article. Review.
-
Manganese-Enhanced Magnetic Resonance Imaging of the Heart.J Magn Reson Imaging. 2023 Apr;57(4):1011-1028. doi: 10.1002/jmri.28499. Epub 2022 Oct 31. J Magn Reson Imaging. 2023. PMID: 36314991 Free PMC article. Review.
Cited by
-
Induced Pluripotent Stem Cell (iPSC)-Derived Exosomes for Precision Medicine in Heart Failure.Circ Res. 2018 Mar 2;122(5):661-663. doi: 10.1161/CIRCRESAHA.118.312657. Circ Res. 2018. PMID: 29496797 Free PMC article. Review. No abstract available.
-
Angiogenic stem cell delivery platform to augment post-infarction neovasculature and reverse ventricular remodeling.Sci Rep. 2022 Oct 20;12(1):17605. doi: 10.1038/s41598-022-21510-y. Sci Rep. 2022. PMID: 36266453 Free PMC article.
-
Growth hormone-releasing hormone agonists reduce myocardial infarct scar in swine with subacute ischemic cardiomyopathy.J Am Heart Assoc. 2015 Mar 31;4(4):e001464. doi: 10.1161/JAHA.114.001464. J Am Heart Assoc. 2015. PMID: 25827134 Free PMC article.
-
Ultra-high field cardiac MRI in large animals and humans for translational cardiovascular research.Front Cardiovasc Med. 2023 May 15;10:1068390. doi: 10.3389/fcvm.2023.1068390. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37255709 Free PMC article.
-
Paracrine Effects of the Pluripotent Stem Cell-Derived Cardiac Myocytes Salvage the Injured Myocardium.Circ Res. 2017 Sep 1;121(6):e22-e36. doi: 10.1161/CIRCRESAHA.117.310803. Epub 2017 Jul 25. Circ Res. 2017. PMID: 28743804 Free PMC article.
References
-
- Cameron A, Davis KB, Green G, Schaff HV. Coronary bypass surgery with internal-thoracic-artery grafts--effects on survival over a 15-year period. N Engl J Med. 1996;334:216–219. - PubMed
-
- Cameron AA, Green GE, Brogno DA, Thornton J. Internal thoracic artery grafts: 20-year clinical follow-up. J Am Coll Cardiol. 1995;25:188–192. - PubMed
-
- Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome: angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J Am Coll Cardiol. 1996;28:616–626. - PubMed
-
- Lytle BW, Cosgrove DM, Loop FD, Borsh J, Goormastic M, Taylor PC. Perioperative risk of bilateral internal mammary artery grafting: analysis of 500 cases from 1971 to 1984. Circulation. 1986;74:III37–41. - PubMed
-
- Kanderian AS, Renapurkar R, Flamm SD. Myocardial viability and revascularization. Heart Fail Clin. 2009;5:333–348. vi. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
