

Near-infrared fluorescence imaging in patients undergoing pancreaticoduodenectomy
- PMID: 21720166
- PMCID: PMC3130979
- DOI: 10.1159/000329411
Near-infrared fluorescence imaging in patients undergoing pancreaticoduodenectomy
Abstract
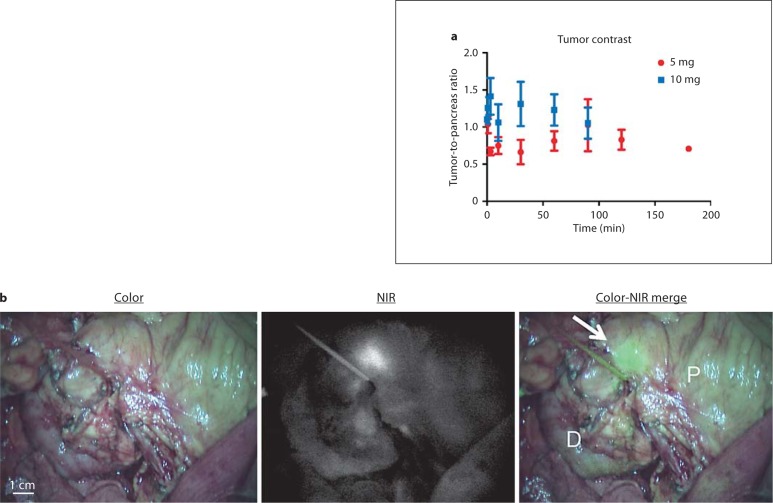
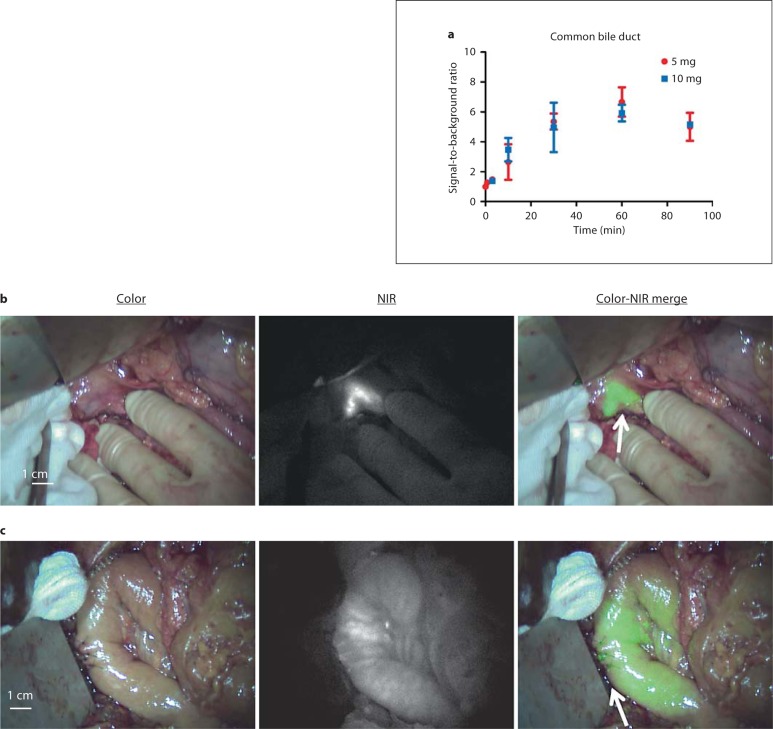
Background: Intraoperative visualization of pancreatic tumors has the potential to improve radical resection rates. Intraoperative visualization of the common bile duct and bile duct anastomoses could be of added value. In this study, we explored the use of indocyanine green (ICG) for these applications and attempted to optimize injection timing and dose.
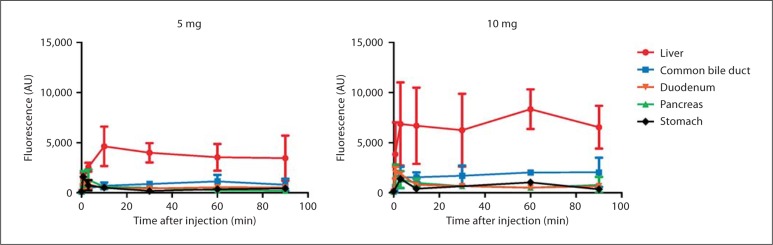
Methods: Eight patients undergoing a pancreaticoduodenectomy were injected intravenously with 5 or 10 mg ICG. During and after injection, the pancreas, tumor, common bile duct and surrounding organs were imaged in real time using the Mini-FLARE™ near-infrared (NIR) imaging system.
Results: No clear tumor-to-pancreas contrast was observed, except for incidental contrast in 1 patient. The common bile duct was clearly visualized using NIR fluorescence, within 10 min after injection, with a maximal contrast between 30 and 90 min after injection. Patency of biliary anastomoses could be visualized due to biliary excretion of ICG.
Conclusion: No useful tumor demarcation could be visualized in pancreatic cancer patients after intravenous injection of ICG. However, the common bile duct and biliary anastomoses were clearly visualized during the observation period. Therefore, these imaging strategies could be beneficial during biliary surgery in cases where the surgical anatomy is aberrant or difficult to identify.
Copyright © 2011 S. Karger AG, Basel.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, Sauter PK, Coleman J, Hruban RH, Lillemoe KD. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
-
- Cleary SP, Gryfe R, Guindi M, Greig P, Smith L, Mackenzie R, Strasberg S, Hanna S, Taylor B, Langer B, Gallinger S. Prognostic factors in resected pancreatic adenocarcinoma: analysis of actual 5-year survivors. J Am Coll Surg. 2004;198:722–731. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
