

A standardized protocol to reduce cerebrospinal fluid shunt infection: the Hydrocephalus Clinical Research Network Quality Improvement Initiative
- PMID: 21721884
- PMCID: PMC3153415
- DOI: 10.3171/2011.4.PEDS10551
A standardized protocol to reduce cerebrospinal fluid shunt infection: the Hydrocephalus Clinical Research Network Quality Improvement Initiative
Abstract
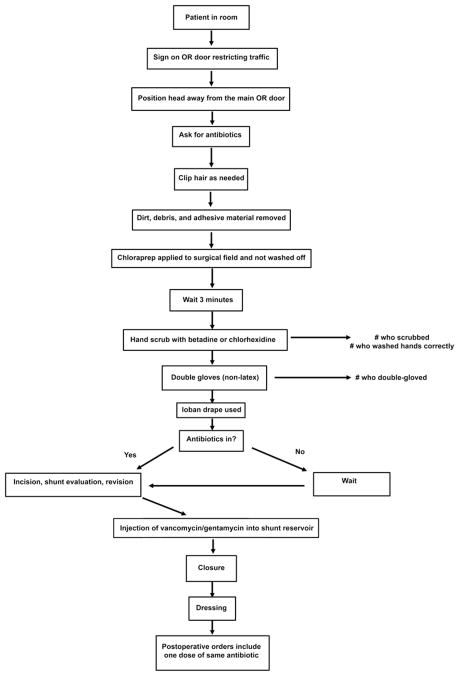
Object: Quality improvement techniques are being implemented in many areas of medicine. In an effort to reduce the ventriculoperitoneal shunt infection rate, a standardized protocol was developed and implemented at 4 centers of the Hydrocephalus Clinical Research Network (HCRN).
Methods: The protocol was developed sequentially by HCRN members using the current literature and prior institutional experience until consensus was obtained. The protocol was prospectively applied at each HCRN center to all children undergoing a shunt insertion or revision procedure. Infections were defined on the basis of CSF, wound, or pseudocyst cultures; wound breakdown; abdominal pseudocyst; or positive blood cultures in the presence of a ventriculoatrial shunt. Procedures and infections were measured before and after protocol implementation.
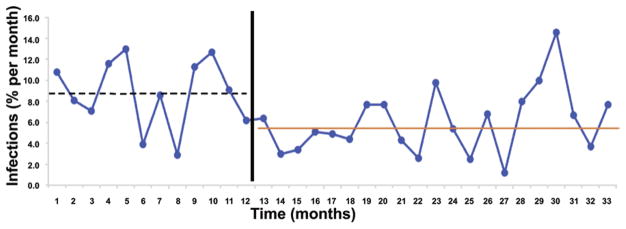
Results: Twenty-one surgeons at 4 centers performed 1571 procedures between June 1, 2007, and February 28, 2009. The minimum follow-up was 6 months. The Network infection rate decreased from 8.8% prior to the protocol to 5.7% while using the protocol (p = 0.0028, absolute risk reduction 3.15%, relative risk reduction 36%). Three of 4 centers lowered their infection rate. Shunt surgery after external ventricular drainage (with or without prior infection) had the highest infection rate. Overall protocol compliance was 74.5% and improved over the course of the observation period. Based on logistic regression analysis, the use of BioGlide catheters (odds ratio [OR] 1.91, 95% CI 1.19-3.05; p = 0.007) and the use of antiseptic cream by any members of the surgical team (instead of a formal surgical scrub by all members of the surgical team; OR 4.53, 95% CI 1.43-14.41; p = 0.01) were associated with an increased risk of infection.
Conclusions: The standardized protocol for shunt surgery significantly reduced shunt infection across the HCRN. Overall protocol compliance was good. The protocol has established a common baseline within the Network, which will facilitate assessment of new treatments. Identification of factors associated with infection will allow further protocol refinement in the future.
Figures
References
-
- Arthur AS, Whitehead WE, Kestle JRW. Duration of antibiotic therapy for the treatment of shunt infection: a surgeon and patient survey. Pediatr Neurosurg. 2002;36:256–259. - PubMed
-
- Cochrane D, Kestle J, Steinbok P, Evans D, Heron N. Model for the cost analysis of shunted hydrocephalic children. Pediatr Neurosurg. 1995;23:14–19. - PubMed
-
- Darouiche RO, Wall MJ, Jr, Itani KM, Otterson MF, Webb AL, Carrick MM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362:18–26. - PubMed
-
- Drake JM. Editorial. Does double gloving prevent cerebrospinal fluid shunt infection? J Neurosurg. 2006;104 (1 Suppl):3–4. - PubMed
-
- Govender ST, Nathoo N, van Dellen JR. Evaluation of an antibiotic- impregnated shunt system for the treatment of hydrocephalus. J Neurosurg. 2003;99:831–839. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
