

Review of electronic decision-support tools for diabetes care: a viable option for low- and middle-income countries?
- PMID: 21722571
- PMCID: PMC3192622
- DOI: 10.1177/193229681100500310
Review of electronic decision-support tools for diabetes care: a viable option for low- and middle-income countries?
Abstract
Context: Diabetes care is complex, requiring motivated patients, providers, and systems that enable guideline-based preventative care processes, intensive risk-factor control, and positive lifestyle choices. However, care delivery in low- and middle-income countries (LMIC) is hindered by a compendium of systemic and personal factors. While electronic medical records (EMR) and computerized clinical decision-support systems (CDSS) have held great promise as interventions that will overcome system-level challenges to improving evidence-based health care delivery, evaluation of these quality improvement interventions for diabetes care in LMICs is lacking. OBJECTIVE AND DATA SOURCES: We reviewed the published medical literature (systematic search of MEDLINE database supplemented by manual searches) to assess the quantifiable and qualitative impacts of combined EMR-CDSS tools on physician performance and patient outcomes and their applicability in LMICs.
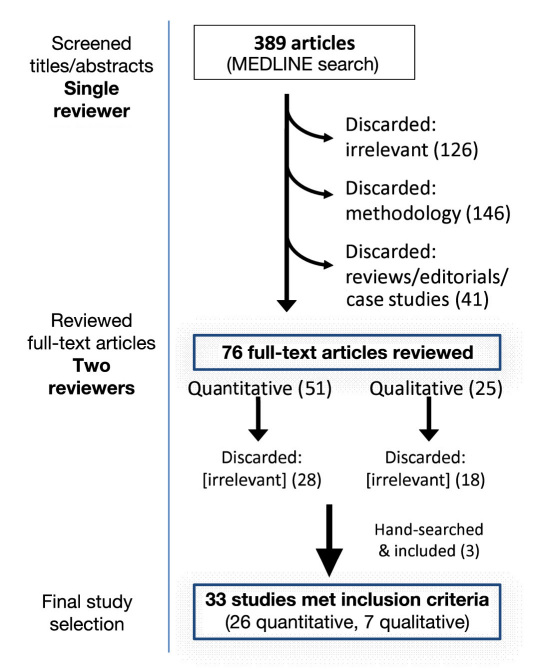
Study selection and data extraction: Inclusion criteria prespecified the population (type 1 or 2 diabetes patients), intervention (clinical EMR-CDSS tools with enhanced functionalities), and outcomes (any process, self-care, or patient-level data) of interest. Case, review, or methods reports and studies focused on nondiabetes, nonclinical, or in-patient uses of EMR-CDSS were excluded. Quantitative and qualitative data were extracted from studies by separate single reviewers, respectively, and relevant data were synthesized.
Results: Thirty-three studies met inclusion criteria, originating exclusively from high-income country settings. Among predominantly experimental study designs, process improvements were consistently observed along with small, variable improvements in risk-factor control, compared with baseline and/or control groups (where applicable). Intervention benefits varied by baseline patient characteristics, features of the EMR-CDSS interventions, motivation and access to technology among patients and providers, and whether EMR-CDSS tools were combined with other quality improvement strategies (e.g., workflow changes, case managers, algorithms, incentives). Patients shared experiences of feeling empowered and benefiting from increased provider attention and feedback but also frustration with technical difficulties of EMR-CDSS tools. Providers reported more efficient and standardized processes plus continuity of care but also role tensions and "mechanization" of care.
Conclusions: This narrative review supports EMR-CDSS tools as innovative conduits for structuring and standardizing care processes but also highlights setting and selection limitations of the evidence reviewed. In the context of limited resources, individual economic hardships, and lack of structured systems or trained human capital, this review reinforces the need for well-designed investigations evaluating the role and feasibility of technological interventions (customized to each LMIC's locality) in clinical decision making for diabetes care.
© 2011 Diabetes Technology Society.
Figures
References
-
- International Diabetes Federation. 4th ed. 2009. Diabetes atlas. www.diabetesatlas.org. - PubMed
-
- Manley SE, Stratton IM, Cull CA, Frighi V, Eeley EA, Matthews DR, Holman RR, Turner RC, Neil HA; United Kingdom Prospective Diabets Study Group. Effects of three months' diet after diagnosis of type 2 diabetes on plasma lipids and lipoproteins (UKPDS 45) Diabet Med. 2000;17(7):518–523. - PubMed
-
- Kris-Etherton P, Eckel RH, Howard BV, St Jeor S, Bazzarre TL; Nutrition Committee Population Science Committee, Clinical Science Committee of the American Heart Association. AHA Science Advisory: Lyon Diet Heart Study. Benefits of a Mediterranean-style, National Cholesterol Education Program/American Heart Association Step I Dietary pattern on cardiovascular disease. Circulation. 2001;103(13):1823–1825. - PubMed
-
- Fletcher GF, Balady GJ, Amsterdam EA, Chaitman B, Eckel R, Fleg J, Froelicher VF, Leon AS, Piña IL, Rodney R, Simons-Morton DA, Williams MA, Bazzarre T. Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation. 2001;104(14):1694–1740. - PubMed
-
- Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, Quyyumi AA, Finkel T. Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N Engl J Med. 2003;348(7):593–600. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
