

Is age-related decline in lean mass and physical function accelerated by obstructive lung disease or smoking?
- PMID: 21724748
- PMCID: PMC3285455
- DOI: 10.1136/thoraxjnl-2011-200010
Is age-related decline in lean mass and physical function accelerated by obstructive lung disease or smoking?
Abstract
Background: and aims Cross-sectional studies suggest that obstructive lung disease (OLD) and smoking affect lean mass and mobility. A study was undertaken to investigate whether OLD and smoking accelerate the ageing-related decline in lean mass and physical functioning.
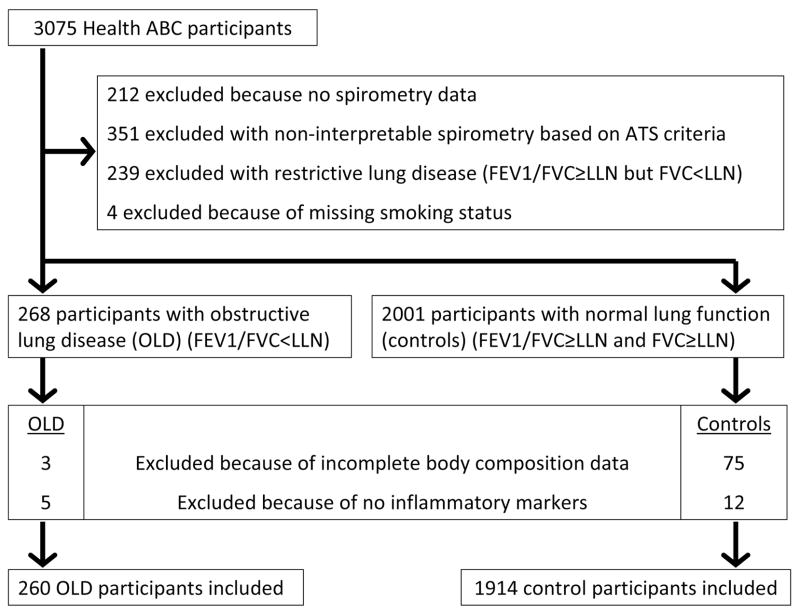
Methods: 260 patients with OLD (mean±SD forced expiratory volume in 1 s (FEV1) 63±18% predicted), 157 smoking controls (FEV(1) 95±16% predicted), 866 former-smoking controls (FEV1 100±16% predicted) and 891 never-smoking controls (FEV1 104±17% predicted) participating in the Health, Aging and Body Composition (ABC) Study were studied. At baseline the mean age was 74±3 years and participants reported no functional limitations. Baseline and 7-year longitudinal data of body composition (by dual-energy x-ray absorptiometry), muscle strength (by hand and leg dynamometry) and Short Physical Performance Battery (SPPB) were investigated.
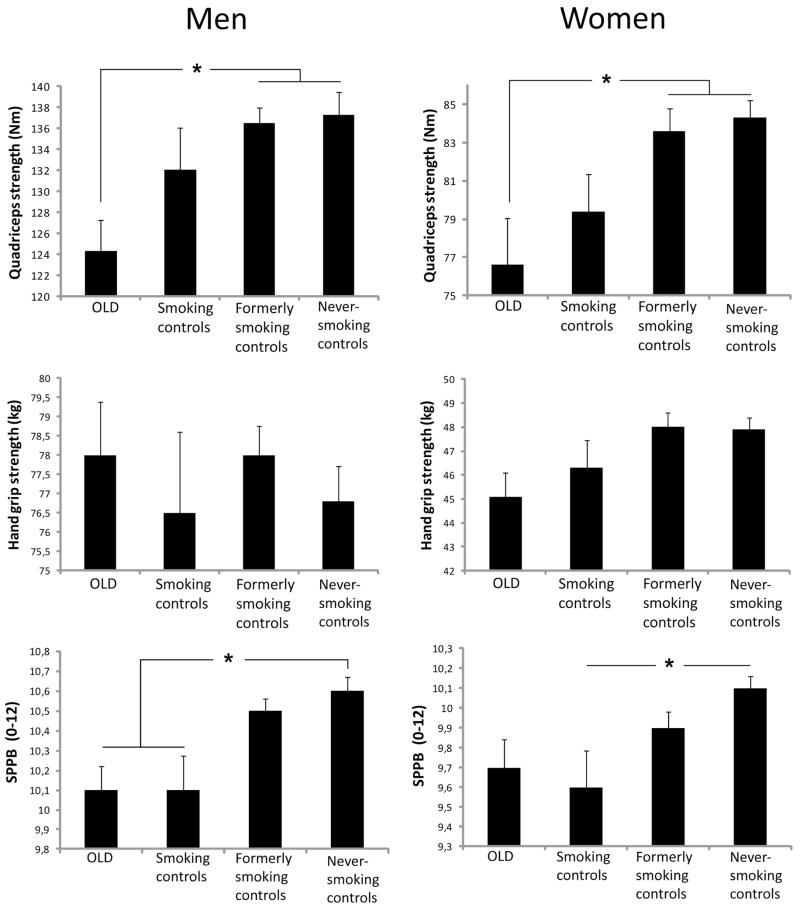
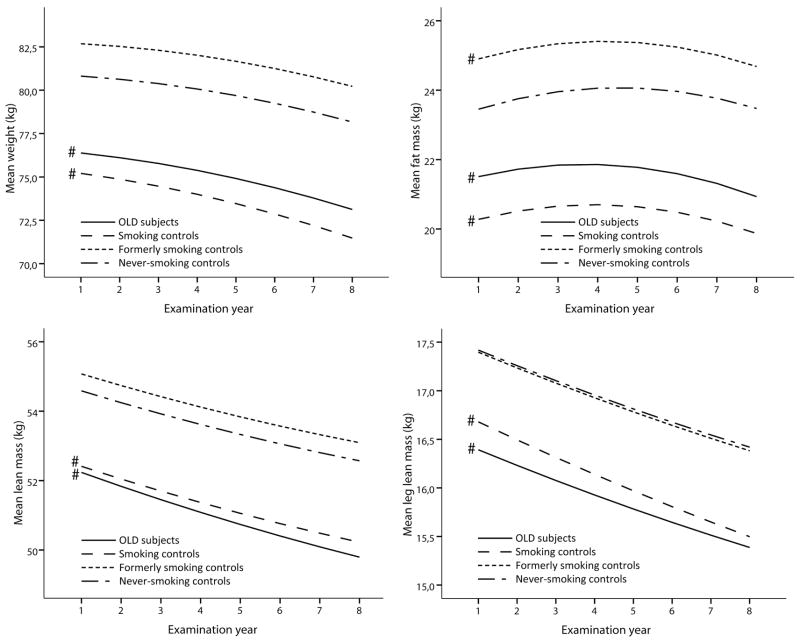
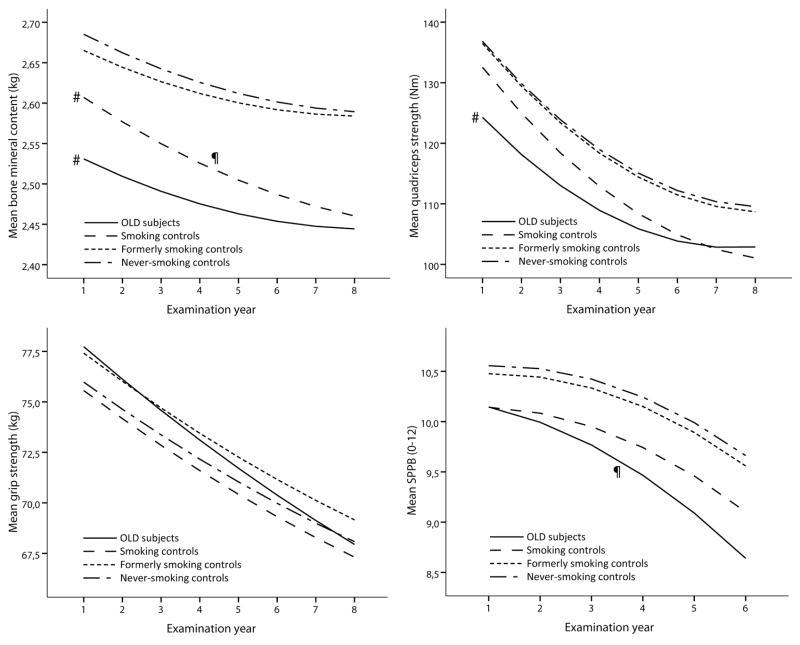
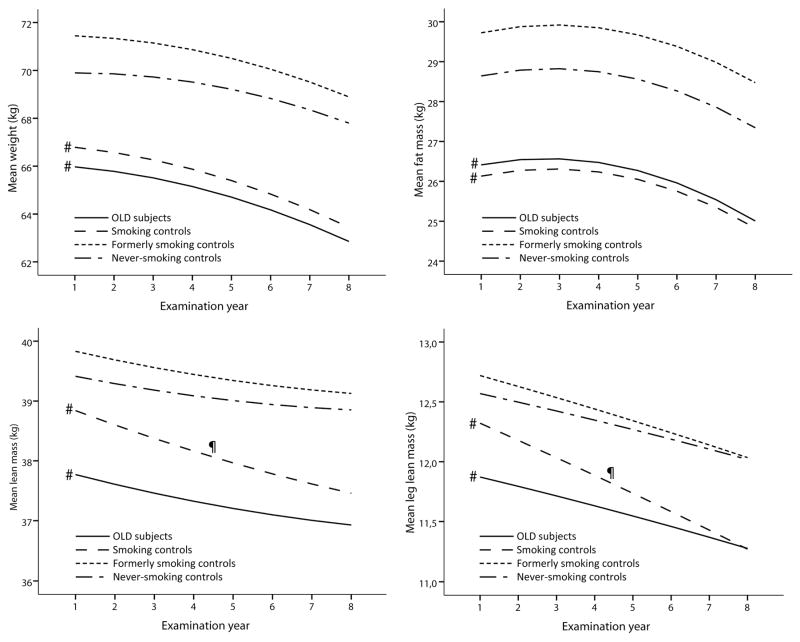
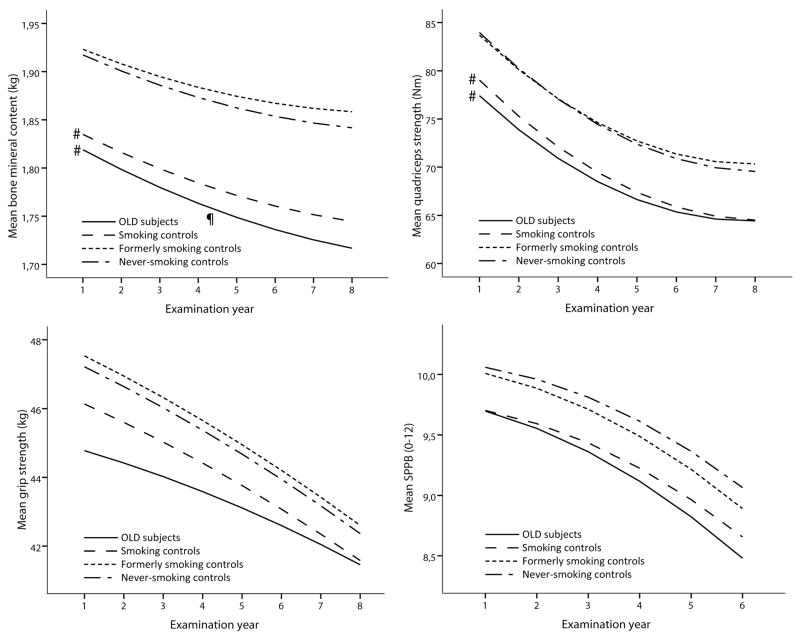
Results: Compared with never-smoking controls, patients with OLD and smoking controls had a significantly lower weight, fat mass, lean mass and bone mineral content (BMC) at baseline (p<0.05). While the loss of weight, fat mass, lean mass and strength was comparable between patients with OLD and never-smoking controls, the SPPB declined 0.12 points/year faster in men with OLD (p=0.01) and BMC declined 4 g/year faster in women with OLD (p=0.02). In smoking controls only lean mass declined 0.1 kg/year faster in women (p=0.03) and BMC 8 g/year faster in men (p=0.02) compared with never-smoking controls.
Conclusions: Initially well-functioning older adults with mild-to-moderate OLD and smokers without OLD have a comparable compromised baseline profile of body composition and physical functioning, while 7-year longitudinal trajectories are to a large extent comparable to those observed in never-smokers without OLD. This suggests a common insult earlier in life related to smoking.
Figures

Comment in
-
Muscle mass and strength in obstructive lung disease: a smoking gun?Thorax. 2011 Nov;66(11):933-5. doi: 10.1136/thoraxjnl-2011-200774. Epub 2011 Aug 3. Thorax. 2011. PMID: 21813620 No abstract available.
References
-
- Gooneratne NS, Patel NP, Corcoran A. Chronic Obstructive Pulmonary Disease diagnosis and management in older adults. Journal of the American Geriatrics Society. 2010;58:1153–62. - PubMed
-
- Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004 Jun;23(6):932–46. - PubMed
-
- Wouters EF, Reynaert NL, Dentener MA, Vernooy JH. Systemic and local inflammation in asthma and chronic obstructive pulmonary disease: is there a connection? Proceedings of the American Thoracic Society. 2009 Dec;6(8):638–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical