

Host response to translocated microbial products predicts outcomes of patients with HBV or HCV infection
- PMID: 21726511
- PMCID: PMC3186837
- DOI: 10.1053/j.gastro.2011.06.063
Host response to translocated microbial products predicts outcomes of patients with HBV or HCV infection
Abstract
Background & aims: Chronic infection with hepatitis B or C virus (HBV or HCV) is a leading cause of cirrhosis by unknown mechanisms of pathogenesis. Translocation of gut microbial products into the systemic circulation might increase because of increased intestinal permeability, bacterial overgrowth, or impaired clearance of microbial products by Kupffer cells. We investigated whether the extent and progression of liver disease in patients with chronic HBV or HCV infection are associated with microbial translocation and subsequent activation of monocytes.
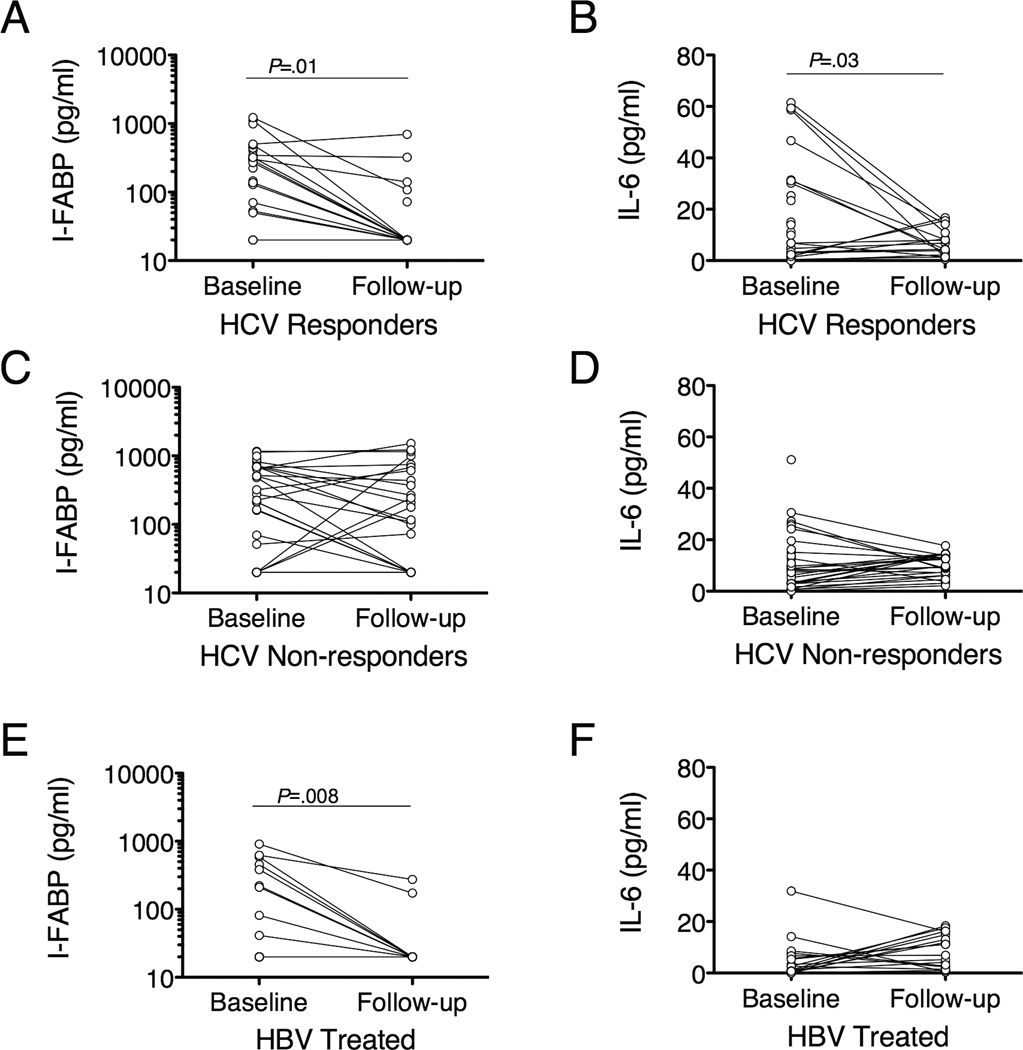
Methods: In a retrospective study, we analyzed data from 16 patients with minimal fibrosis, 68 with cirrhosis, and 67 uninfected volunteers. We analyzed plasma levels of soluble CD14 (sCD14), intestinal fatty acid binding protein, and interleukin-6 by enzyme-linked immunosorbent assay, and lipopolysaccharide (LPS) by the limulus amebocyte lysate assay, at presentation and after antiviral treatment.
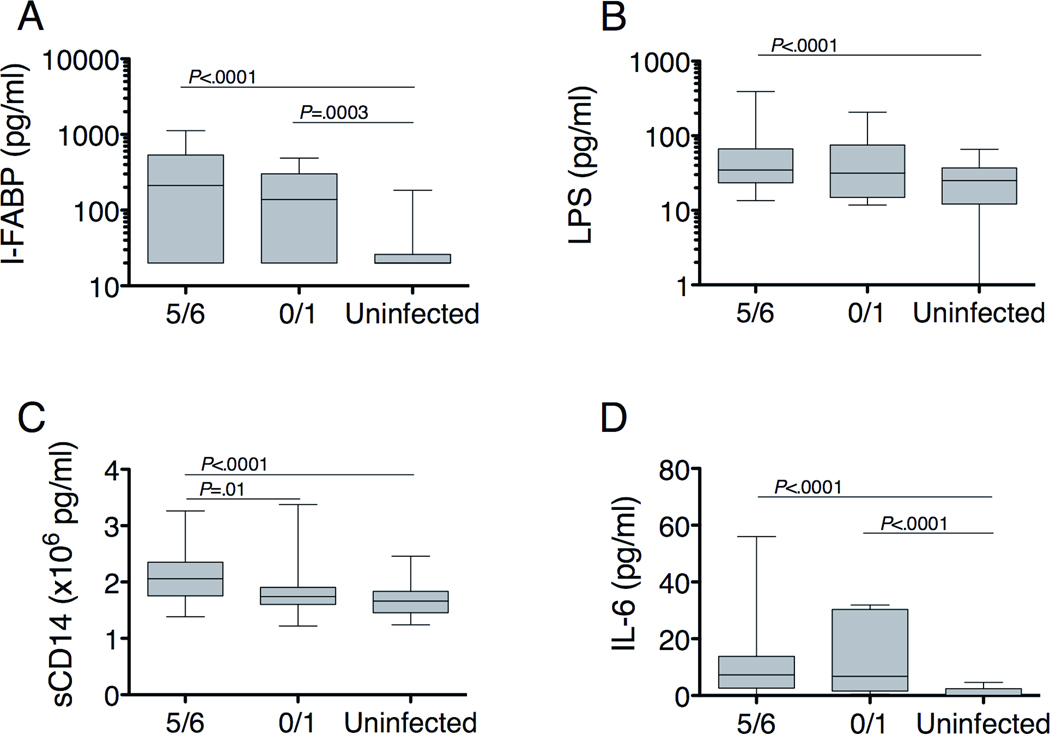
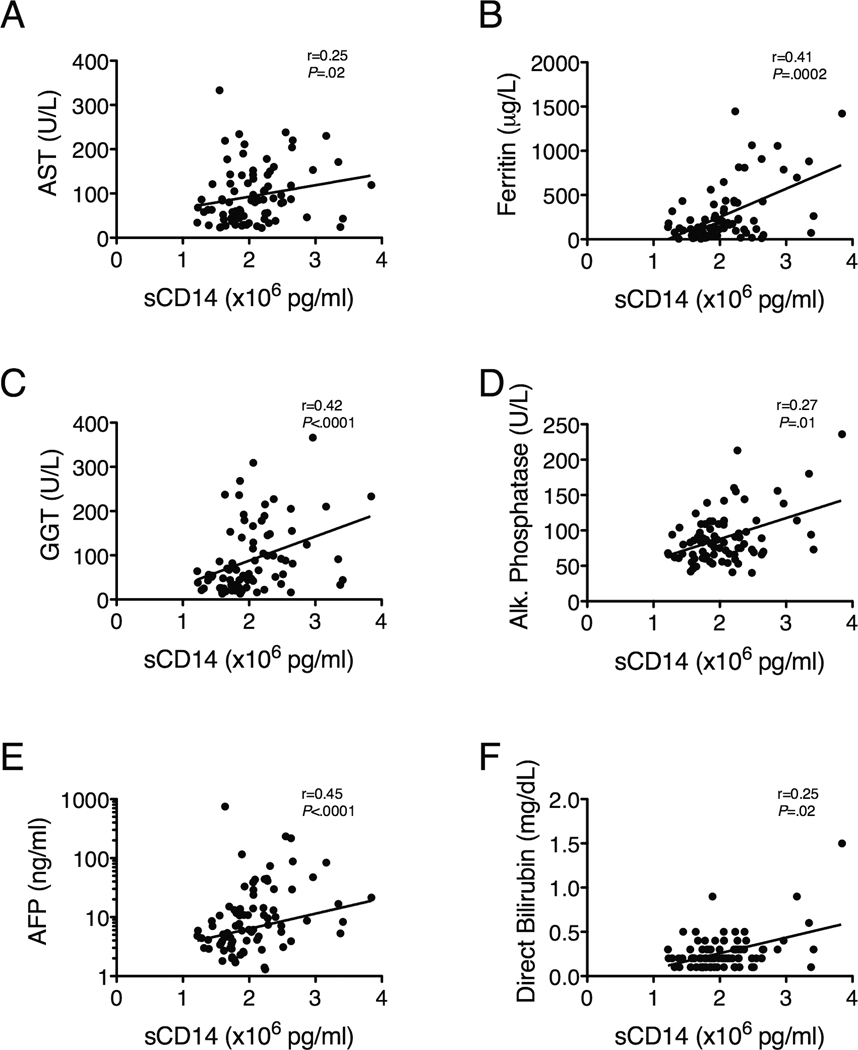
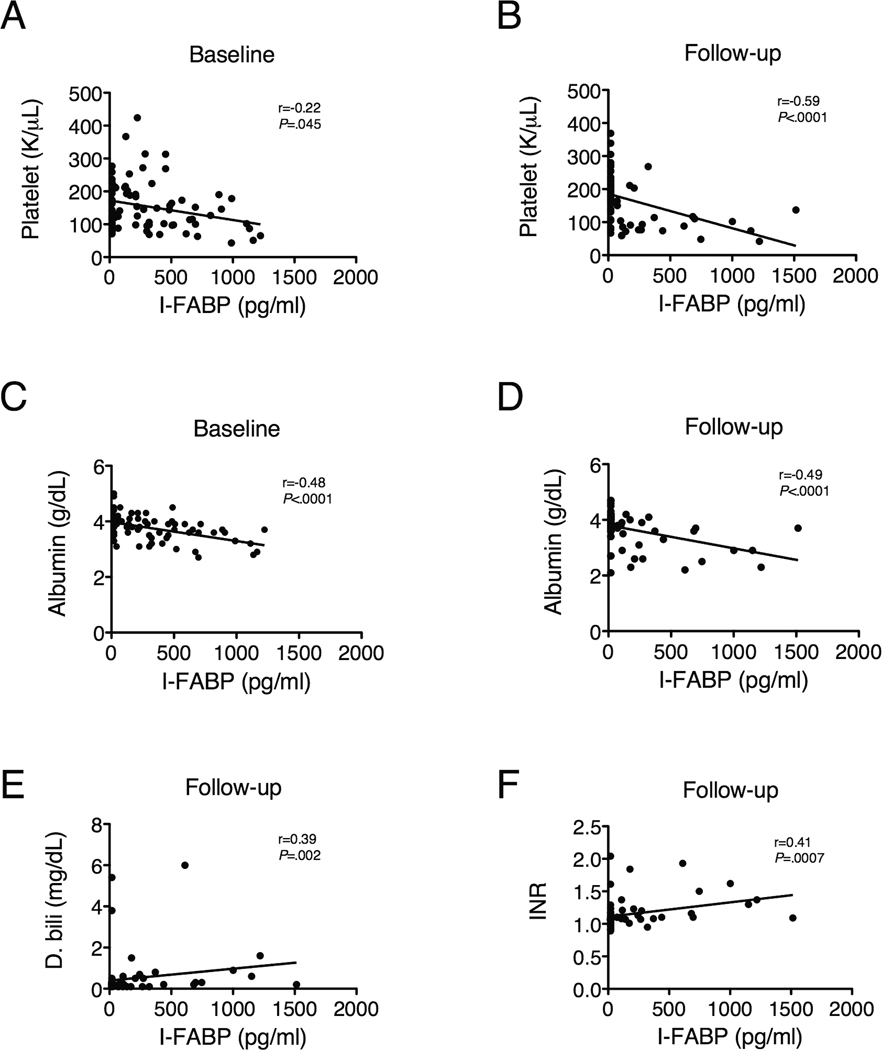
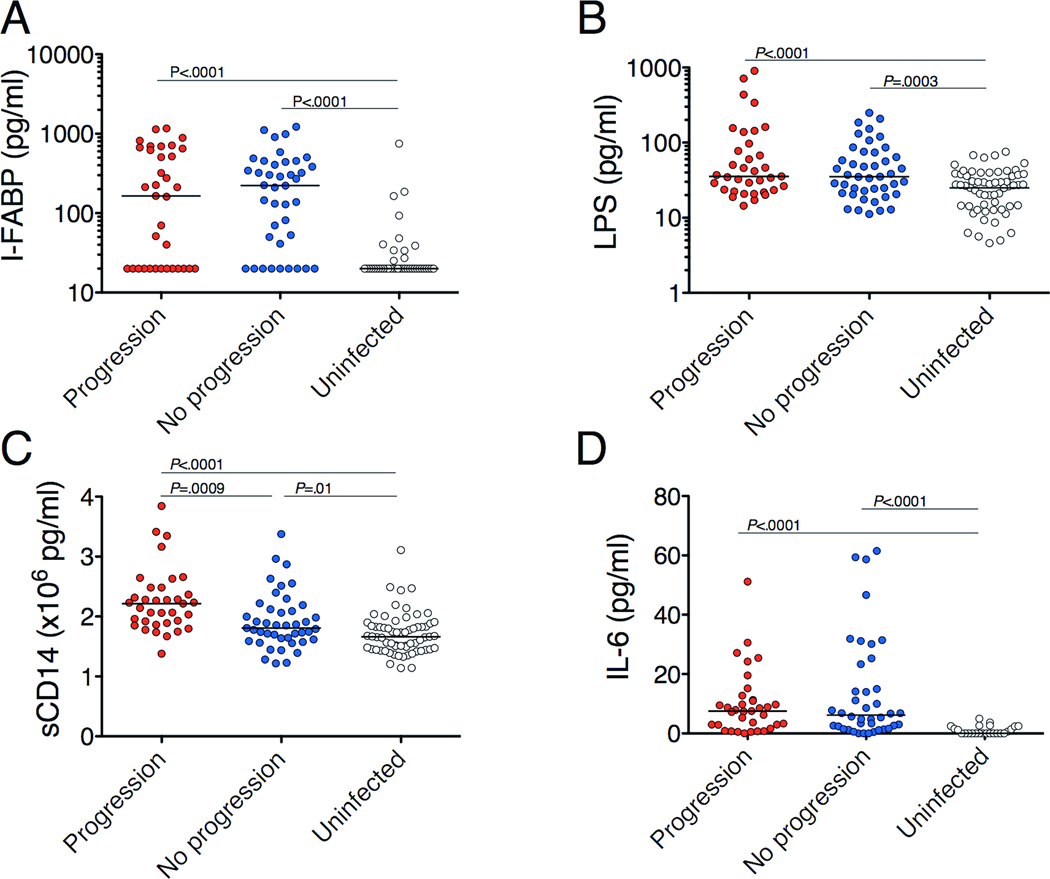
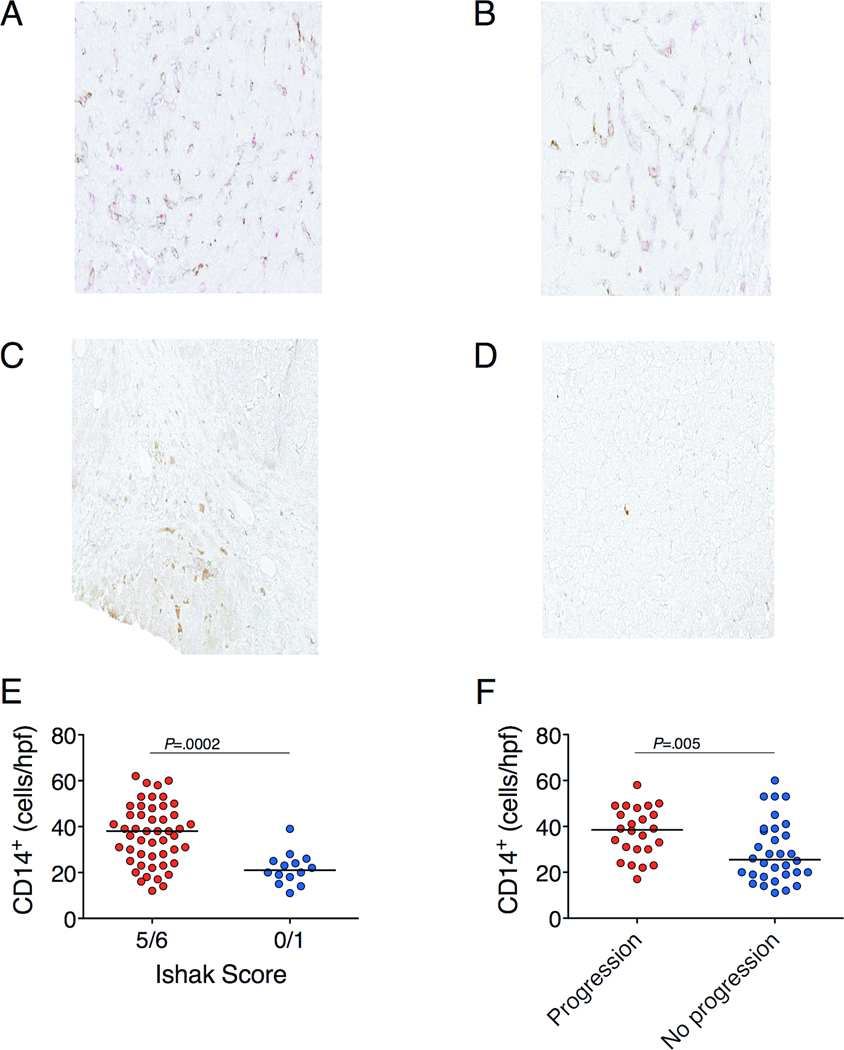
Results: Compared with uninfected individuals, HCV- and HBV-infected individuals had higher plasma levels of LPS, intestinal fatty acid binding protein (indicating enterocyte death), sCD14 (produced upon LPS activation of monocytes), and interleukin-6. Portal hypertension, indicated by low platelet counts, was associated with enterocyte death (P=.045 at presentation, P<.0001 after therapy). Levels of sCD14 correlated with markers of hepatic inflammation (P=.02 for aspartate aminotransferase, P=.002 for ferritin) and fibrosis (P<.0001 for γ-glutamyl transpeptidase, P=.01 for alkaline phosphatase, P<.0001 for α-fetoprotein). Compared to subjects with minimal fibrosis, subjects with severe fibrosis at presentation had higher plasma levels of sCD14 (P=.01) and more hepatic CD14+ cells (P=.0002); each increased risk for disease progression (P=.0009 and P=.005, respectively).
Conclusions: LPS-induced local and systemic inflammation is associated with cirrhosis and predicts progression to end-stage liver disease in patients with HBV or HCV infection.
Copyright © 2011 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Jirillo E, Caccavo D, Magrone T, et al. The role of the liver in the response to LPS: experimental and clinical findings. J Endotoxin Res. 2002;8:319–327. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
