

Personalizing mammography by breast density and other risk factors for breast cancer: analysis of health benefits and cost-effectiveness
- PMID: 21727289
- PMCID: PMC3759993
- DOI: 10.7326/0003-4819-155-1-201107050-00003
Personalizing mammography by breast density and other risk factors for breast cancer: analysis of health benefits and cost-effectiveness
Abstract
Background: Current guidelines recommend mammography every 1 or 2 years starting at age 40 or 50 years, regardless of individual risk for breast cancer.
Objective: To estimate the cost-effectiveness of mammography by age, breast density, history of breast biopsy, family history of breast cancer, and screening interval.
Design: Markov microsimulation model.
Data sources: Surveillance, Epidemiology, and End Results program, Breast Cancer Surveillance Consortium, and the medical literature.
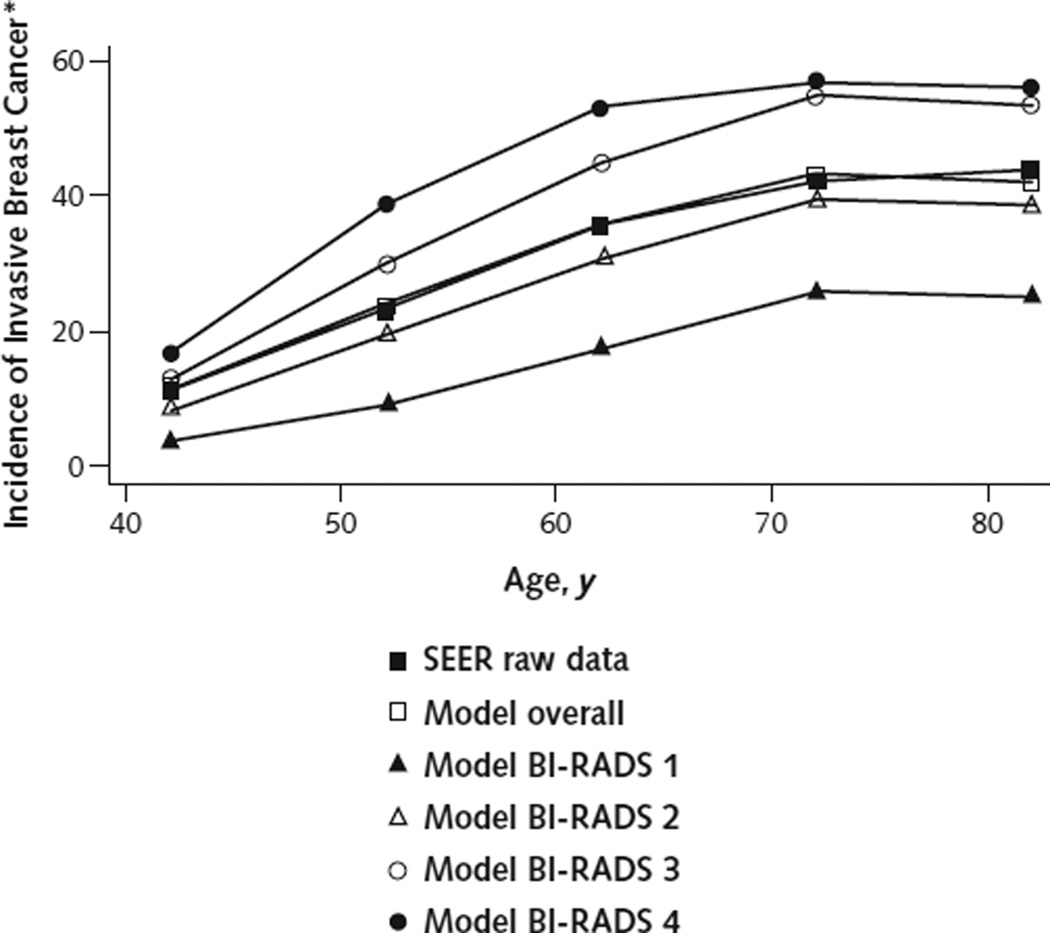
Target population: U.S. women aged 40 to 49, 50 to 59, 60 to 69, and 70 to 79 years with initial mammography at age 40 years and breast density of Breast Imaging Reporting and Data System (BI-RADS) categories 1 to 4.
Time horizon: Lifetime.
Perspective: National health payer.
Intervention: Mammography annually, biennially, or every 3 to 4 years or no mammography.
Outcome measures: Costs per quality-adjusted life-year (QALY) gained and number of women screened over 10 years to prevent 1 death from breast cancer.
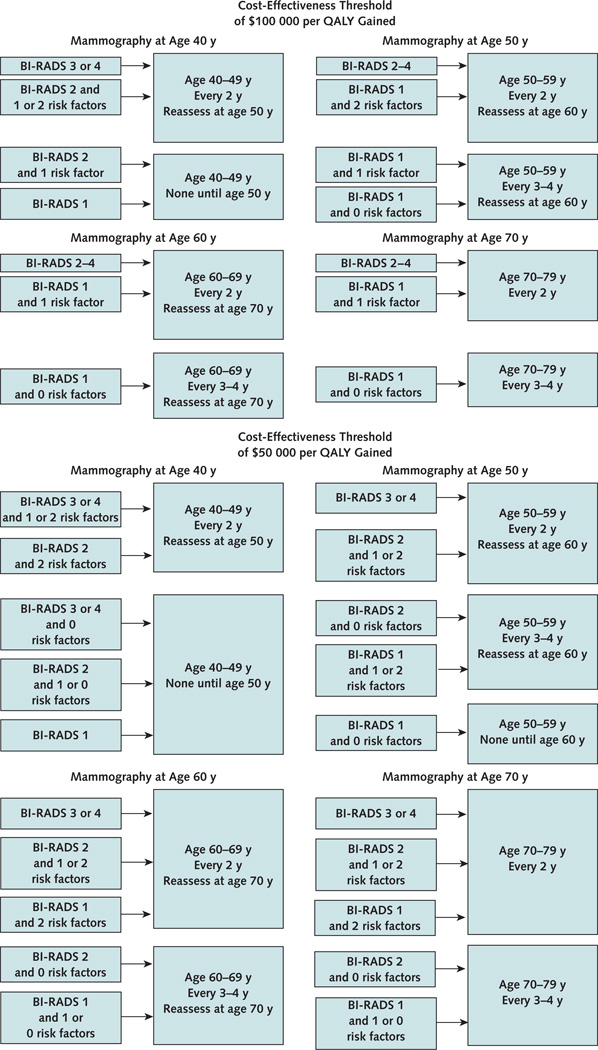
Results of base-case analysis: Biennial mammography cost less than $100,000 per QALY gained for women aged 40 to 79 years with BI-RADS category 3 or 4 breast density or aged 50 to 69 years with category 2 density; women aged 60 to 79 years with category 1 density and either a family history of breast cancer or a previous breast biopsy; and all women aged 40 to 79 years with both a family history of breast cancer and a previous breast biopsy, regardless of breast density. Biennial mammography cost less than $50,000 per QALY gained for women aged 40 to 49 years with category 3 or 4 breast density and either a previous breast biopsy or a family history of breast cancer. Annual mammography was not cost-effective for any group, regardless of age or breast density.
Results of sensitivity analysis: Mammography is expensive if the disutility of false-positive mammography results and the costs of detecting nonprogressive and nonlethal invasive cancer are considered.
Limitation: Results are not applicable to carriers of BRCA1 or BRCA2 mutations.
Conclusion: Mammography screening should be personalized on the basis of a woman's age, breast density, history of breast biopsy, family history of breast cancer, and beliefs about the potential benefit and harms of screening.
Primary funding source: Eli Lilly, Da Costa Family Foundation for Research in Breast Cancer Prevention of the California Pacific Medical Center, and Breast Cancer Surveillance Consortium.
Conflict of interest statement
Figures

Comment in
-
To screen or not to screen women in their 40s for breast cancer: is personalized risk-based screening the answer?Ann Intern Med. 2011 Jul 5;155(1):58-60. doi: 10.7326/0003-4819-155-1-201107050-00008. Ann Intern Med. 2011. PMID: 21727294 No abstract available.
-
Analysis of health benefits and cost-effectiveness of mammography for breast cancer.Ann Intern Med. 2011 Oct 18;155(8):566; author reply 566-7. doi: 10.7326/0003-4819-155-8-201110180-00028. Ann Intern Med. 2011. PMID: 22007057 No abstract available.
References
-
- Lee CH. Screening mammography: proven benefit, continued controversy. Radiol Clin North Am. 2002;40:395–407. [PMID: 12117183] - PubMed
-
- Sirovich BE, Sox HC., Jr. Breast cancer screening. Surg Clin North Am. 1999;79:961–990. [PMID: 10572546] - PubMed
-
- Berry DA, Cronin KA, Plevritis SK, Fryback DG, Clarke L, Zelen M, et al. Cancer Intervention and Surveillance Modeling Network (CISNET) Collaborators. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784–1792. [PMID: 16251534] - PubMed
-
- Gøtzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev. 2006:CD001877. [PMID: 17054145] - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA69976/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous