

Dose-response relationship between alcohol consumption before and during pregnancy and the risks of low birthweight, preterm birth and small for gestational age (SGA)-a systematic review and meta-analyses
- PMID: 21729235
- PMCID: PMC3394156
- DOI: 10.1111/j.1471-0528.2011.03050.x
Dose-response relationship between alcohol consumption before and during pregnancy and the risks of low birthweight, preterm birth and small for gestational age (SGA)-a systematic review and meta-analyses
Abstract
Background: Descriptions of the effects of moderate alcohol consumption during pregnancy on adverse pregnancy outcomes have been inconsistent.
Objective: To review systematically and perform meta-analyses on the effect of maternal alcohol exposure on the risk of low birthweight, preterm birth and small for gestational age (SGA).
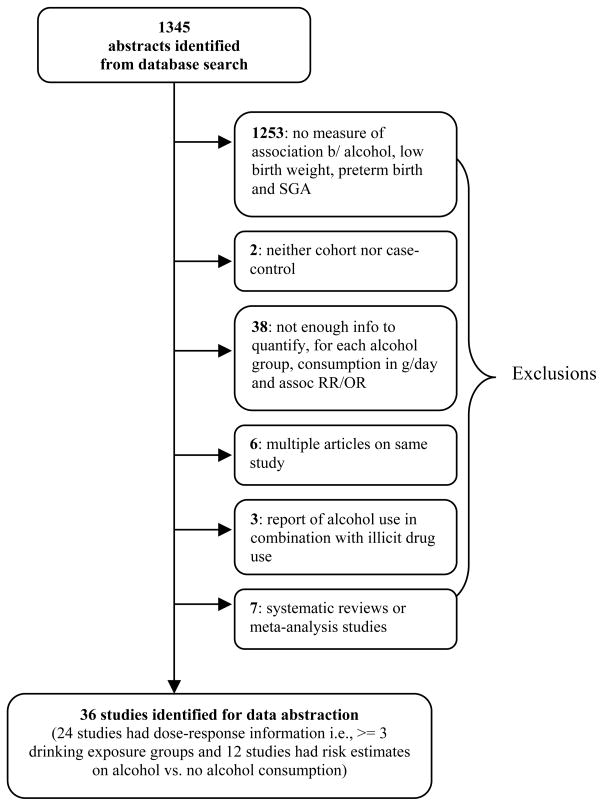
Search strategy: Using Medical Subject Headings, a literature search of MEDLINE, EMBASE, CINAHL, CABS, WHOlist, SIGLE, ETOH, and Web of Science between 1 January 1980 and 1 August 2009 was performed followed by manual searches.
Selection criteria: Case-control or cohort studies were assessed for quality (STROBE), 36 available studies were included.
Data collection and analysis: Two reviewers independently extracted the information on low birthweight, preterm birth and SGA using a standardised protocol. Meta-analyses on dose-response relationships were performed using linear as well as first-order and second-order fractional polynomial regressions to estimate best fitting curves to the data.
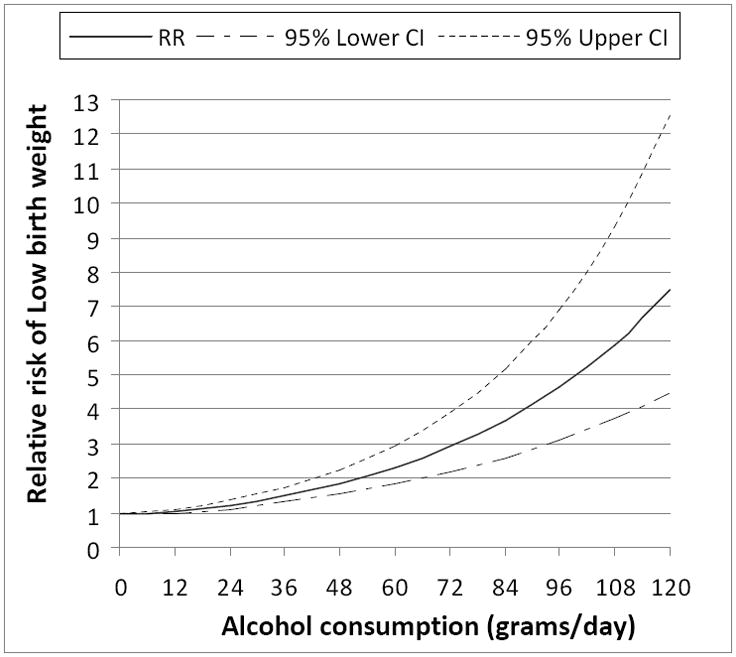
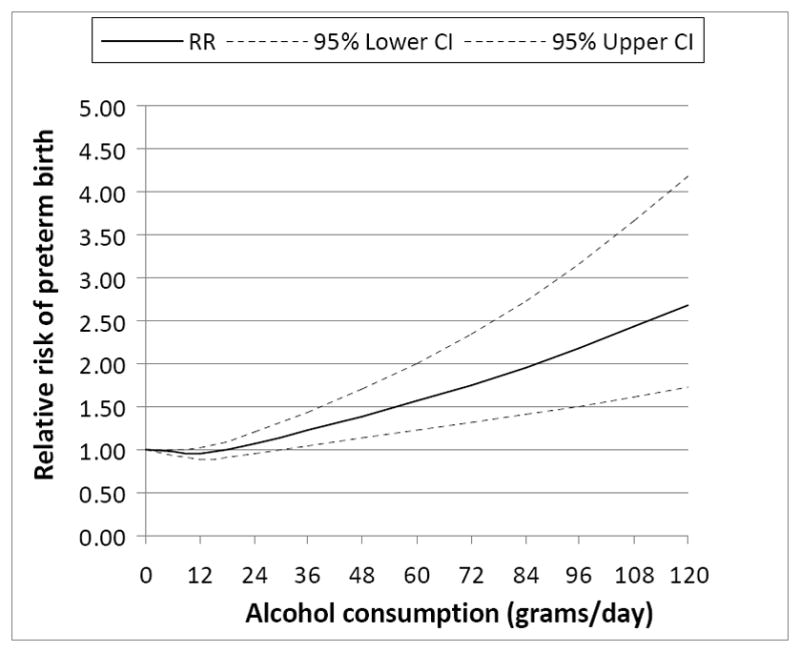
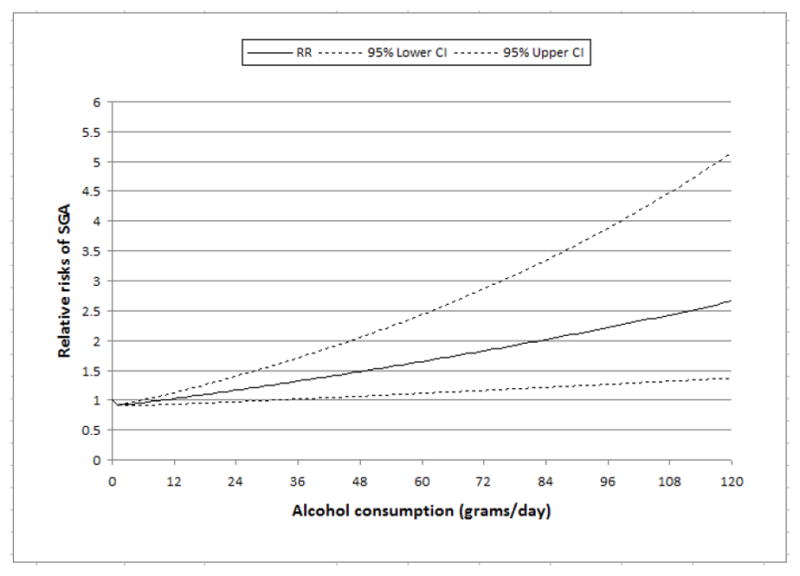
Main results: Compared with abstainers, the overall dose-response relationships for low birthweight and SGA showed no effect up to 10 g pure alcohol/day (an average of about 1 drink/day) and preterm birth showed no effect up to 18 g pure alcohol/day (an average of 1.5 drinks/day); thereafter, the relationship showed a monotonically increasing risk for increasing maternal alcohol consumption. Moderate consumption during pre-pregnancy was associated with reduced risks for all outcomes.
Conclusions: Dose-response relationship indicates that heavy alcohol consumption during pregnancy increases the risks of all three outcomes whereas light to moderate alcohol consumption shows no effect. Preventive measures during antenatal consultations should be initiated.
© 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology © 2011 RCOG.
Conflict of interest statement
Figures

Comment in
-
The association between prenatal alcohol exposure, fetal growth and preterm birth: evidence from a systematic review and meta-analyses.Evid Based Nurs. 2012 Jul;15(3):77-8. doi: 10.1136/ebnurs-2012-100516. Epub 2012 Apr 25. Evid Based Nurs. 2012. PMID: 22535581 No abstract available.
References
-
- Sokol RJ, Delaney-Black V, Nordstrom B. Fetal alcohol spectrum disorder. JAMA. 2003;290:2996–2999. - PubMed
-
- Barr HM, Bookstein FL, O’Malley KD, Connor PD, Huggins JE, Streissguth AP. Binge drinking during pregnancy as a predictor of psychiatric disorders on the Structured Clinical Interview for DSM-IV in young adult offspring. Am J Psychiatry. 2006;163:1061–1065. - PubMed
-
- Hanson JW, Streissguth AP, Smith DW. The effect of moderate alcohol consumption during pregnancy on fetal growth and morphogenesis. Journal of Pediatrics. 1978;92:457–460. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
