

The effects of melatonin versus placebo on delirium in hip fracture patients: study protocol of a randomised, placebo-controlled, double blind trial
- PMID: 21729284
- PMCID: PMC3148574
- DOI: 10.1186/1471-2318-11-34
The effects of melatonin versus placebo on delirium in hip fracture patients: study protocol of a randomised, placebo-controlled, double blind trial
Abstract
Background: With an ageing population, older persons become a larger part of the hospital population. The incidence of delirium is high in this group, and experiencing delirium has major short- and long-term sequelae, which makes prevention crucial. During delirium, a disruption of the sleep-wake cycle is frequently observed. Melatonin plays an important role in the regulation of the sleep-wake cycle, so this raised the hypothesis that alterations in the metabolism of melatonin might play an important role in the development of delirium. The aim of this article is to describe the design of a randomised, placebo controlled double-blind trial that is currently in progress and that investigates the effects of melatonin versus placebo on delirium in older, postoperative hip fracture patients.
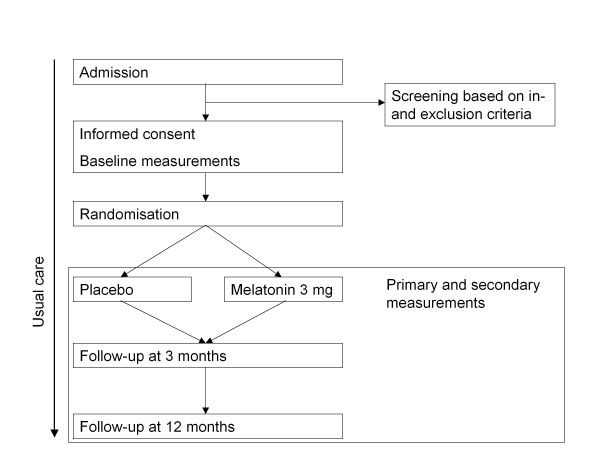
Methods/design: Acutely hospitalised patients aged 65 years or older admitted for surgical repair of hip fracture are randomised (n=452) into a treatment or placebo group. Prophylactic treatment consists of orally administered melatonin (3 mg) at 21:00 h on five consecutive days. The primary outcome is the occurrence of delirium, to be diagnosed according to the Confusion Assessment Method, within eight days after start of the study medication. Secondary outcomes are delirium severity, measured by the Delirium Rating Scale; duration of delirium; differences in subtypes of delirium; differences in total length of hospital stay; total dose of antipsychotics and/or benzodiazepine use during delirium; and in-hospital complications. In the twelve-month follow up visit, cognitive function is measured by a Mini-Mental state examination and the Informant Questionnaire on Cognitive Decline in the Elderly. Functional status is assessed with the Katz ADL index score (patient and family version) and grip strength measurement. The outcomes of these assessments are compared to the outcomes that were obtained during admission.
Discussion: The proposed study will contribute to our knowledge because studies on the prophylactic treatment of delirium with long term follow up remain scarce. The results may lead to a prophylactic treatment for frail older persons at high risk for delirium that is safe, effective, and easily implementable in daily practice.
Trial registration: Dutch Clinical Trial Registry: NTR1576.
Figures
References
-
- van Munster BC, Korevaar JC, Zwinderman AH, Levi M, Wiersinga WJ, de Rooij SE. Time-Course of Cytokines During Delirium in Elderly Patients with Hip Fractures. J Am Geriatr Soc. 2008. - PubMed
-
- Siddiqi N, Stockdale R, Britton AM, Holmes J. Interventions for preventing delirium in hospitalised patients. Cochrane Database Syst Rev. 2007. p. CD005563. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
