

Association between provision of mental illness beds and rate of involuntary admissions in the NHS in England 1988-2008: ecological study
- PMID: 21729994
- PMCID: PMC3130113
- DOI: 10.1136/bmj.d3736
Association between provision of mental illness beds and rate of involuntary admissions in the NHS in England 1988-2008: ecological study
Abstract
Objective: To examine the rise in the rate of involuntary admissions for mental illness in England that has occurred as community alternatives to hospital admission have been introduced.
Design: Ecological analysis.
Setting: England, 1988-2008.
Data source: Publicly available data on provision of beds for people with mental illness in the National Health Service from Hospital Activity Statistics and involuntary admission rates from the NHS Information Centre.
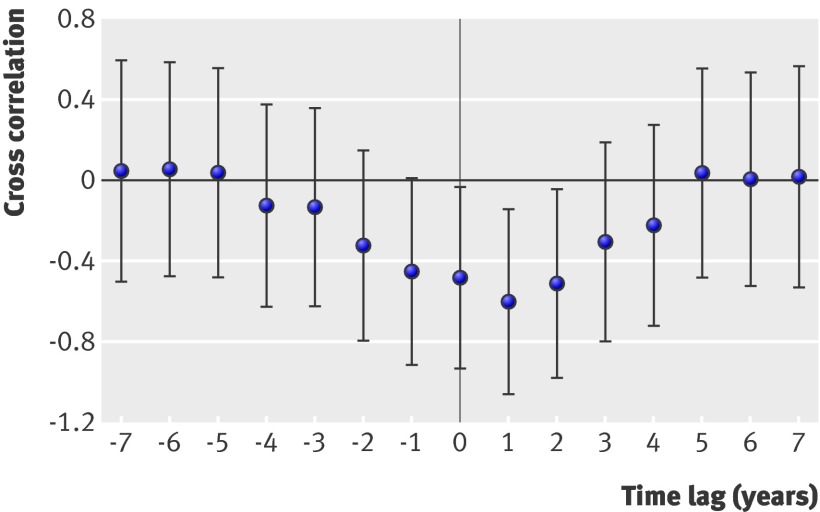
Main outcome measures: Association between annual changes in provision of mental illness beds in the NHS and involuntary admission rates, using cross correlation. Partial correlation coefficients were calculated and regression analysis carried out for the time lag (interval) over which the largest association between these variables was identified.
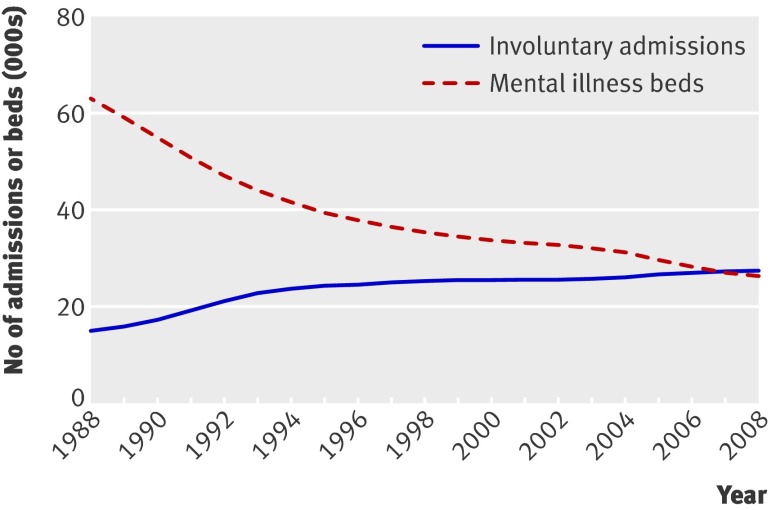
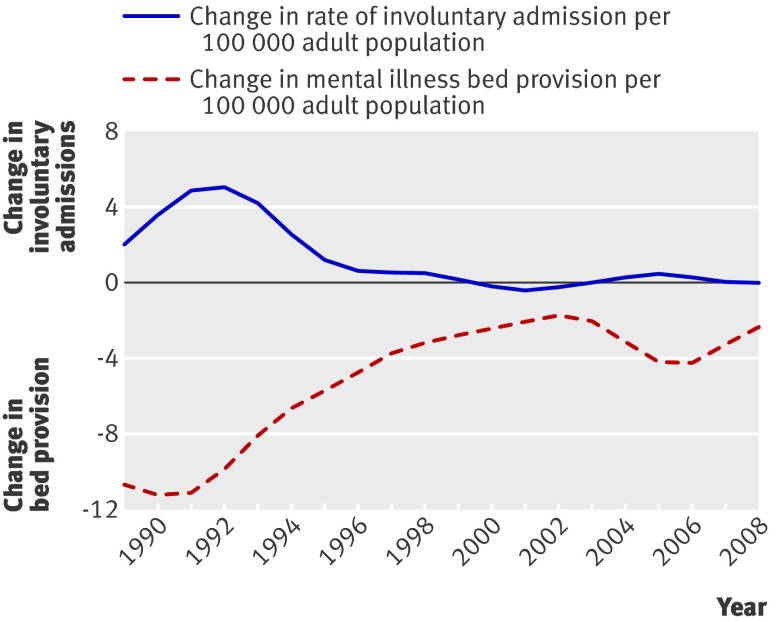
Results: The rate of involuntary admissions per annum in the NHS increased by more than 60%, whereas the provision of mental illness beds decreased by more than 60% over the same period; these changes seemed to be synchronous. The strongest association between these variables was observed when a time lag of one year was introduced, with bed reductions preceding increases in involuntary admissions (cross correlation -0.60, 95% confidence interval -1.06 to -0.15). This association increased in magnitude when analyses were restricted to civil (non-forensic) involuntary admissions and non-secure mental illness beds.
Conclusion: The annual reduction in provision of mental illness beds was associated with the rate of involuntary admissions over the short to medium term, with the closure of two mental illness beds leading to one additional involuntary admission in the subsequent year. This study provides a method for predicting rates of involuntary admissions and what may happen in the future if bed closures continue.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical