

Quality of care and patient outcomes in critical access rural hospitals
- PMID: 21730240
- PMCID: PMC3337777
- DOI: 10.1001/jama.2011.902
Quality of care and patient outcomes in critical access rural hospitals
Abstract
Context: Critical access hospitals (CAHs) play a crucial role in the US rural safety net. Current policy efforts have focused primarily on helping these small, isolated hospitals remain financially viable to ensure access for individuals living in rural areas in the United States; however, little is known about the quality of care they provide or the outcomes their patients achieve.
Objectives: To examine the quality of care and patient outcomes at CAHs and to understand why patterns of care might differ for CAHs vs non-CAHs.
Design, setting, and patients: A retrospective analysis in 4738 US hospitals of Medicare fee-for-service beneficiaries with acute myocardial infarction (AMI) (10,703 for CAHs vs 469,695 for non-CAHs), congestive heart failure (CHF) (52,927 for CAHs vs 958,790 for non-CAHs), and pneumonia (86,359 for CAHs vs 773,227 for non-CAHs) who were discharged in 2008-2009.
Main outcome measures: Clinical capabilities, performance on processes of care, and 30-day mortality rates, adjusted for age, sex, race, and medical comorbidities.
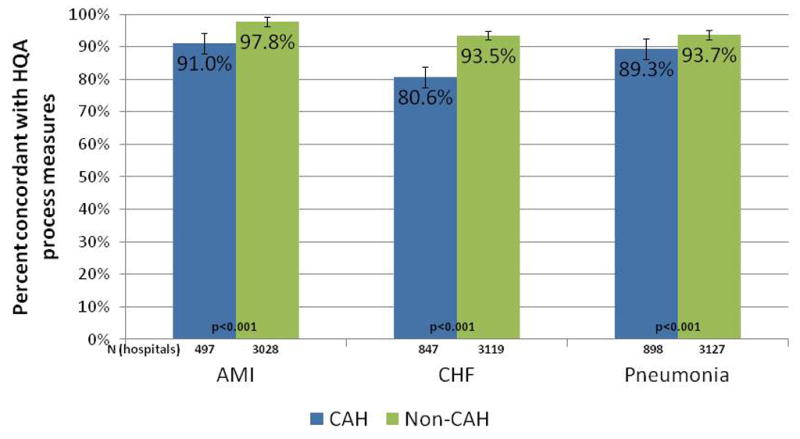
Results: Compared with other hospitals (n = 3470), 1268 CAHs (26.8%) were less likely to have intensive care units (380 [30.0%] vs 2581 [74.4%], P < .001), cardiac catheterization capabilities (6 [0.5%] vs 1654 [47.7%], P < .001), and at least basic electronic health records (80 [6.5%] vs 445 [13.9%], P < .001). The CAHs had lower performance on processes of care than non-CAHs for all 3 conditions examined (concordance with Hospital Quality Alliance process measures for AMI, 91.0% [95% CI, 89.7%-92.3%] vs 97.8% [95% CI, 97.7%-97.9%]; for CHF, 80.6% [95% CI, 79.2%-82.0%] vs 93.5% [95% CI, 93.3%-93.7%]; and for pneumonia, 89.3% [95% CI, 88.6%-90.0%] vs 93.7% [95% CI, 93.6%-93.9%]; P < .001 for each). Patients admitted to CAHs had higher 30-day mortality rates for each condition than those admitted to non-CAHs (for AMI: 23.5% vs 16.2%; adjusted odds ratio [OR], 1.70; 95% confidence interval [CI], 1.61-1.80; P < .001; for CHF: 13.4% vs 10.9%; adjusted OR, 1.28; 95% CI, 1.23-1.32; P < .001; and for pneumonia: 14.1% vs 12.1%; adjusted OR, 1.20; 95% CI, 1.16-1.24; P < .001).
Conclusion: Compared with non-CAHs, CAHs had fewer clinical capabilities, worse measured processes of care, and higher mortality rates for patients with AMI, CHF, or pneumonia.
Conflict of interest statement
Dr. Joynt has no conflicts to declare. Dr. Harris has no conflicts to declare. Dr. Orav has no conflicts to declare. Dr. Jha has no relevant conflicts; he has provided consulting support to UpToDate and is on the Scientific Advisory Board for Humedica.
Figures
Comment in
-
Critical access hospitals and the challenges to quality care.JAMA. 2011 Jul 6;306(1):96-7. doi: 10.1001/jama.2011.928. JAMA. 2011. PMID: 21730248 No abstract available.
-
Quality of care in critical access hospitals.JAMA. 2011 Oct 19;306(15):1653; author reply 1654-5. doi: 10.1001/jama.2011.1487. JAMA. 2011. PMID: 22009094 No abstract available.
-
Quality of care in critical access hospitals.JAMA. 2011 Oct 19;306(15):1653-4; author reply 1654-5. doi: 10.1001/jama.2011.1488. JAMA. 2011. PMID: 22009095 No abstract available.
-
Quality of care in critical access hospitals.JAMA. 2011 Oct 19;306(15):1654; author reply 1654-5. doi: 10.1001/jama.2011.1489. JAMA. 2011. PMID: 22009096 No abstract available.
References
-
-
The Balanced Budget Act of 1997. HR 2015; 1997.
-
-
- Medicare Payment Advisory Committee. Report to the Congress: Issues in a Modernized Medicare Program. Washington, D.C: MedPAC; 2005.
-
- Stensland J, Davidson G, Moscovice I. The Financial Benefits of Critical Access Conversion: Working Paper 44. Minneapolis, MN: University of Minnesota Rural Health Research Center; 2004.
-
- U.S. Census Bureau. Census 2000 Summary File Data. U.S. Census Bureau; 2000.
-
- Casey MM, Davidson G. Upper Midwest Rural Health Research Center Final Report #10: Patient Assessments and Quality of Care in Rural Hospitals. Minneapolis, MN: Upper Midwest Rural Health Research Center, University of Minnesota; 2010.
