

Appropriateness of percutaneous coronary intervention
- PMID: 21730241
- PMCID: PMC3293218
- DOI: 10.1001/jama.2011.916
Appropriateness of percutaneous coronary intervention
Abstract
Context: Despite the widespread use of percutaneous coronary intervention (PCI), the appropriateness of these procedures in contemporary practice is unknown.
Objective: To assess the appropriateness of PCI in the United States.
Design, setting, and patients: Multicenter, prospective study of patients within the National Cardiovascular Data Registry undergoing PCI between July 1, 2009, and September 30, 2010, at 1091 US hospitals. The appropriateness of PCI was adjudicated using the appropriate use criteria for coronary revascularization. Results were stratified by whether the procedure was performed for an acute (ST-segment elevation myocardial infarction, non-ST-segment elevation myocardial infarction, or unstable angina with high-risk features) or nonacute indication.
Main outcome measures: Proportion of acute and nonacute PCIs classified as appropriate, uncertain, or inappropriate; extent of hospital-level variation in inappropriate procedures.
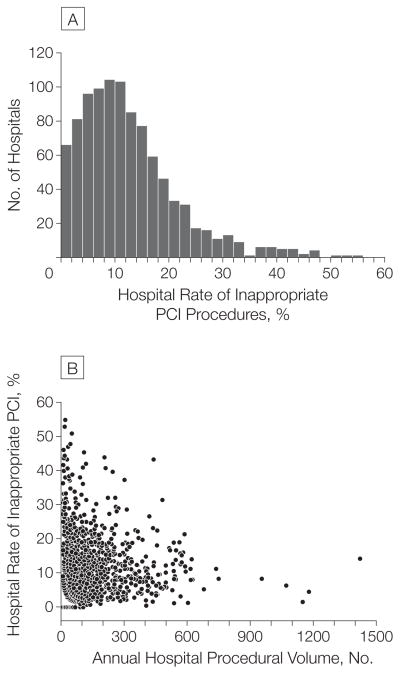
Results: Of 500,154 PCIs, 355,417 (71.1%) were for acute indications (ST-segment elevation myocardial infarction, 103,245 [20.6%]; non-ST-segment elevation myocardial infarction, 105,708 [21.1%]; high-risk unstable angina, 146,464 [29.3%]), and 144,737 (28.9%) for nonacute indications. For acute indications, 350,469 PCIs (98.6%) were classified as appropriate, 1055 (0.3%) as uncertain, and 3893 (1.1%) as inappropriate. For nonacute indications, 72,911 PCIs (50.4%) were classified as appropriate, 54,988 (38.0%) as uncertain, and 16,838 (11.6%) as inappropriate. The majority of inappropriate PCIs for nonacute indications were performed in patients with no angina (53.8%), low-risk ischemia on noninvasive stress testing (71.6%), or suboptimal (≤1 medication) antianginal therapy (95.8%). Furthermore, although variation in the proportion of inappropriate PCI across hospitals was minimal for acute procedures, there was substantial hospital variation for nonacute procedures (median hospital rate for inappropriate PCI, 10.8%; interquartile range, 6.0%-16.7%).
Conclusions: In this large contemporary US cohort, nearly all acute PCIs were classified as appropriate. For nonacute indications, however, 12% were classified as inappropriate, with substantial variation across hospitals.
Conflict of interest statement
Figures

Comment in
-
Underuse of percutaneous coronary intervention.JAMA. 2011 Nov 16;306(19):2094; author reply 2094-5. doi: 10.1001/jama.2011.1658. JAMA. 2011. PMID: 22089715 No abstract available.
-
Assessing appropriateness of coronary intervention.Rev Cardiovasc Med. 2011;12(3):170-1. Rev Cardiovasc Med. 2011. PMID: 22145194 No abstract available.
References
-
- Cadet J. AHA adjusts angioplasty stats to lower annual figure. [Accessed January 20, 2011];Cardiovascular Business Web site. 2010 December 19; http://www.cardiovascularbusiness.com/index.php?option=com_articles&arti....
-
- Mahoney EM, Wang K, Arnold SV, et al. Cost-effectiveness of prasugrel versus clopidogrel in patients with acute coronary syndromes and planned percutaneous coronary intervention: results from the trial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel—Thrombolysis in Myocardial Infarction TRITON-TIMI 38. Circulation. 2010;121(1):71–79. - PubMed
-
- Boden WE, O’Rourke RA, Teo KK, et al. COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503–1516. - PubMed
-
- Hilborne LH, Leape LL, Bernstein SJ, et al. The appropriateness of use of percutaneous transluminal coronary angioplasty in New York State. JAMA. 1993;269(6):761–765. - PubMed
-
- Yim J, Khang YH, Oh BH, Kim YI, Kim CY. The appropriateness of percutaneous transluminal coronary angioplasty in Korea. Int J Cardiol. 2004;95(2–3):199–205. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
