

The economics of improving medication adherence in osteoporosis: validation and application of a simulation model
- PMID: 21733991
- PMCID: PMC3167669
- DOI: 10.1210/jc.2011-0575
The economics of improving medication adherence in osteoporosis: validation and application of a simulation model
Abstract
Context: Adherence to osteoporosis treatment is low. Although new therapies and behavioral interventions may improve medication adherence, questions are likely to arise regarding their cost-effectiveness.
Objective: Our objectives were to develop and validate a model to simulate the clinical outcomes and costs arising from various osteoporosis medication adherence patterns among women initiating bisphosphonate treatment and to estimate the cost-effectiveness of a hypothetical intervention to improve medication adherence.
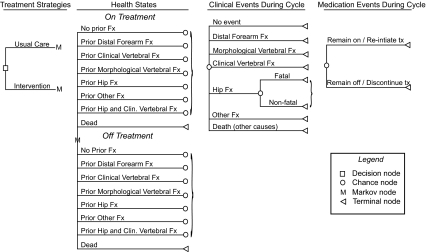
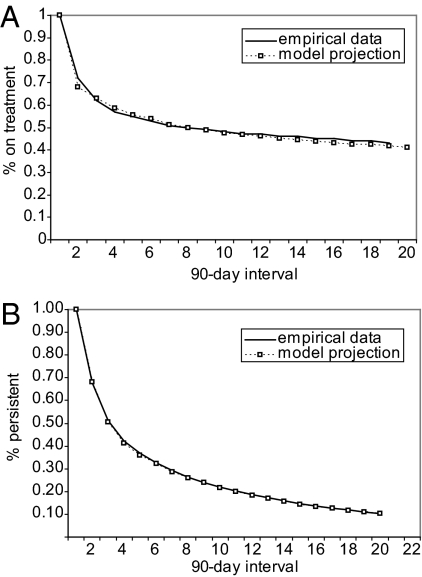
Design: We constructed a computer simulation using estimates of fracture rates, bisphosphonate treatment effects, costs, and utilities for health states drawn from the published literature. Probabilities of transitioning on and off treatment were estimated from administrative claims data.
Setting and patients: Patients were women initiating bisphosphonate therapy from the general community.
Intervention: We evaluated a hypothetical behavioral intervention to improve medication adherence.
Main outcome measures: Changes in 10-yr fracture rates and incremental cost-effectiveness ratios were evaluated.
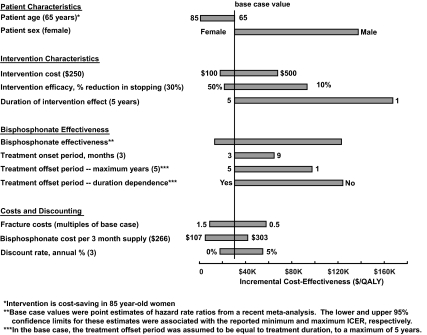
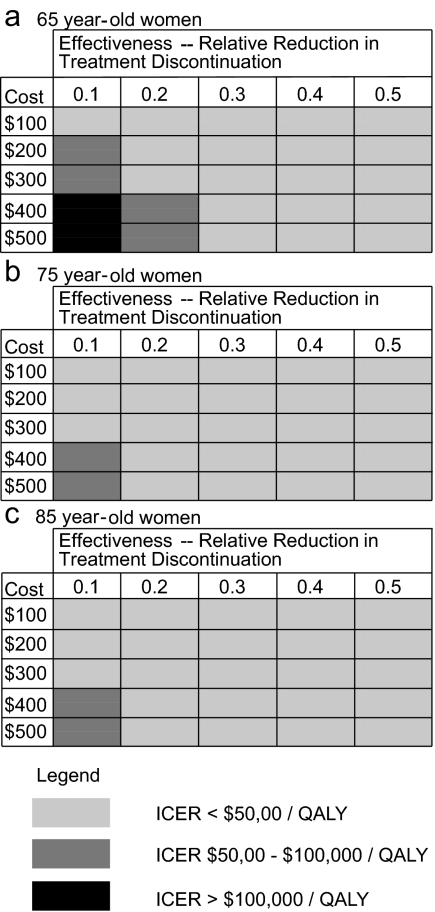
Results: A hypothetical intervention with a one-time cost of $250 and reducing bisphosphonate discontinuation by 30% had an incremental cost-effectiveness ratio (ICER) of $29,571 per quality-adjusted life year in 65-yr-old women initiating bisphosphonates. Although the ICER depended on patient age, intervention effectiveness, and intervention cost, the ICERs were less than $50,000 per quality-adjusted life year for the majority of intervention cost and effectiveness scenarios evaluated. Results were sensitive to bisphosphonate cost and effectiveness and assumptions about the rate at which intervention and treatment effects decline over time.
Conclusions: Our results suggests that behavioral interventions to improve osteoporosis medication adherence will likely have favorable ICERs if their efficacy can be sustained.
Figures
Similar articles
-
Cost effectiveness of fracture prevention in postmenopausal women who receive aromatase inhibitors for early breast cancer.J Clin Oncol. 2012 May 1;30(13):1468-75. doi: 10.1200/JCO.2011.38.7001. Epub 2012 Feb 27. J Clin Oncol. 2012. PMID: 22370313
-
Cost-effectiveness of bisphosphonate therapies for women with postmenopausal osteoporosis: implications of improved persistence with less frequently administered oral bisphosphonates.Curr Med Res Opin. 2007 Oct;23(10):2517-29. doi: 10.1185/030079907X226339. Curr Med Res Opin. 2007. PMID: 17825128 Clinical Trial.
-
The cost effectiveness of teriparatide as a first-line treatment for glucocorticoid-induced and postmenopausal osteoporosis patients in Sweden.BMC Musculoskelet Disord. 2012 Oct 30;13:213. doi: 10.1186/1471-2474-13-213. BMC Musculoskelet Disord. 2012. PMID: 23110626 Free PMC article.
-
The cost effectiveness of bisphosphonates for the prevention and treatment of osteoporosis: a structured review of the literature.Pharmacoeconomics. 2007;25(11):913-33. doi: 10.2165/00019053-200725110-00003. Pharmacoeconomics. 2007. PMID: 17960951 Review.
-
Denosumab: A Unique Perspective on Adherence and Cost-effectiveness Compared With Oral Bisphosphonates in Osteoporosis Patients.Ann Pharmacother. 2018 Oct;52(10):1031-1041. doi: 10.1177/1060028018768808. Epub 2018 Apr 4. Ann Pharmacother. 2018. PMID: 29616561 Review.
Cited by
-
Economic evaluation of a population-based osteoporosis intervention for outpatients with non-traumatic non-hip fractures: the "Catch a Break" 1i [type C] FLS.Osteoporos Int. 2017 Jun;28(6):1965-1977. doi: 10.1007/s00198-017-3986-3. Epub 2017 Mar 9. Osteoporos Int. 2017. PMID: 28275838 Free PMC article.
-
Medication adherence and health care utilization in pediatric chronic illness: a systematic review.Pediatrics. 2013 Oct;132(4):730-40. doi: 10.1542/peds.2013-1451. Epub 2013 Sep 2. Pediatrics. 2013. PMID: 23999953 Free PMC article.
-
Health technology assessment in osteoporosis.Calcif Tissue Int. 2013 Jul;93(1):1-14. doi: 10.1007/s00223-013-9724-8. Epub 2013 Mar 21. Calcif Tissue Int. 2013. PMID: 23515633 Free PMC article. Review.
-
Potential cost-effectiveness for using patient decision aids to guide osteoporosis treatment.Osteoporos Int. 2016 Sep;27(9):2697-2707. doi: 10.1007/s00198-016-3596-5. Epub 2016 May 7. Osteoporos Int. 2016. PMID: 27155885
-
The potential economic benefits of improved postfracture care: a cost-effectiveness analysis of a fracture liaison service in the US health-care system.J Bone Miner Res. 2014 Jul;29(7):1667-74. doi: 10.1002/jbmr.2180. J Bone Miner Res. 2014. PMID: 24443384 Free PMC article.
References
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. 2007. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22:465–475 - PubMed
-
- Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P, Rosen C. 2002. Meta-analyses of therapies for postmenopausal osteoporosis. IX: Summary of meta-analyses of therapies for postmenopausal osteoporosis. Endocr Rev 23:570–578 - PubMed
-
- Kothawala P, Badamgarav E, Ryu S, Miller RM, Halbert RJ. 2007. Systematic review and meta-analysis of real-world adherence to drug therapy for osteoporosis. Mayo Clin Proc 82:1493–1501 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
