

Approach to the child with fractures
- PMID: 21734001
- PMCID: PMC3135196
- DOI: 10.1210/jc.2010-2546
Approach to the child with fractures
Abstract
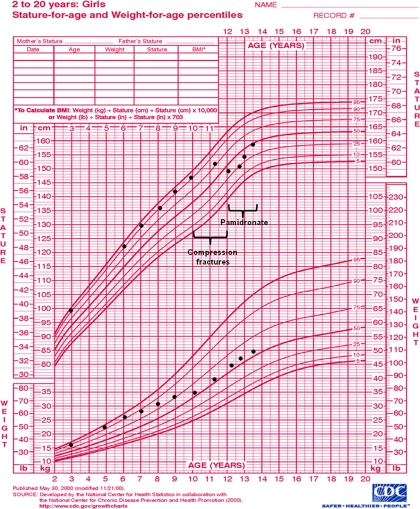
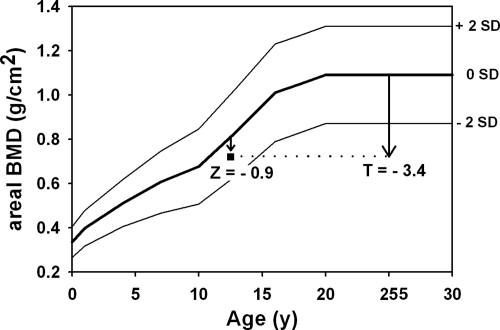
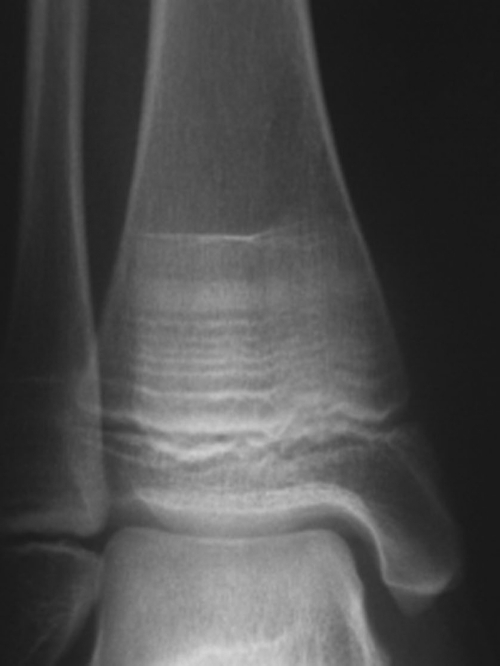
Evaluation of the child with fractures is challenging, as no clear guidelines exist to distinguish traumatic from pathological fractures. Although most fractures in childhood are benign, recurrent fractures may be associated with a wide variety of primary skeletal diseases as well as secondary causes, necessitating a careful history and physical exam to guide the evaluation. There is no "gold standard" for the evaluation and treatment of children with fractures and low bone mineral density (BMD); therefore, the diagnosis of osteoporosis in a pediatric patient should be made using a combination of clinical and radiographic features. Interpretation of bone densitometry in growing patients presents a unique set of challenges because areal BMD measured by dual-energy x-ray absorptiometry depends on multiple dynamic variables. Interpretation of pediatric dual-energy x-ray absorptiometry should be based on Z-scores (sd scores compared to age, sex, and ethnicity-matched controls), using normative databases specific to the brand of densitometer and the patient population. Given the skeleton's ability to recover from low BMD through modeling and remodeling, optimizing management of underlying conditions leading to bone fragility is the initial step. Conservative measures including calcium and vitamin D supplementation and weight-bearing physical activity are important interventions that should not be overlooked. The use of bisphosphonates in children and adolescents is controversial due to lack of long-term efficacy and safety data and should be limited to clinical trials and compassionate therapy in children with significantly compromised quality of life. Close monitoring is required, and further study is necessary to assess their long-term safety and efficacy in children.
Figures
References
-
- Landin LA. 1997. Epidemiology of children's fractures. J Pediatr Orthop B 6:79–83 - PubMed
-
- Jones IE, Williams SM, Dow N, Goulding A. 2002. How many children remain fracture-free during growth? a longitudinal study of children and adolescents participating in the Dunedin Multidisciplinary Health and Development Study. Osteoporos Int 13:990–995 - PubMed
-
- Khosla S, Melton LJ, 3rd, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL. 2003. Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA 290:1479–1485 - PubMed
-
- Mäyränpää MK, Mäkitie O, Kallio PE. 2010. Decreasing incidence and changing pattern of childhood fractures: a population-based study. J Bone Miner Res 25:2476–2483 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
