

Clinical practices and outcomes in elderly hemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS)
- PMID: 21734085
- PMCID: PMC4204107
- DOI: 10.2215/CJN.03530410
Clinical practices and outcomes in elderly hemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS)
Abstract
Background and objectives: Demand for hemodialysis among elderly patients is increasing worldwide. Although clinical care of this high-risk group is complex and challenging, no guidelines exist to inform hemodialysis practices. The Dialysis Outcomes and Practice Patterns Study (DOPPS) provides a unique opportunity to assess dialysis practices and associated outcomes among elderly versus younger patients on chronic in-center hemodialysis in 12 countries.
Design, setting, participants, & measurements: Clinical characteristics, dialysis practices, and outcomes of elderly versus younger patients were compared among participants in four DOPPS regions in 2005 through 2007.
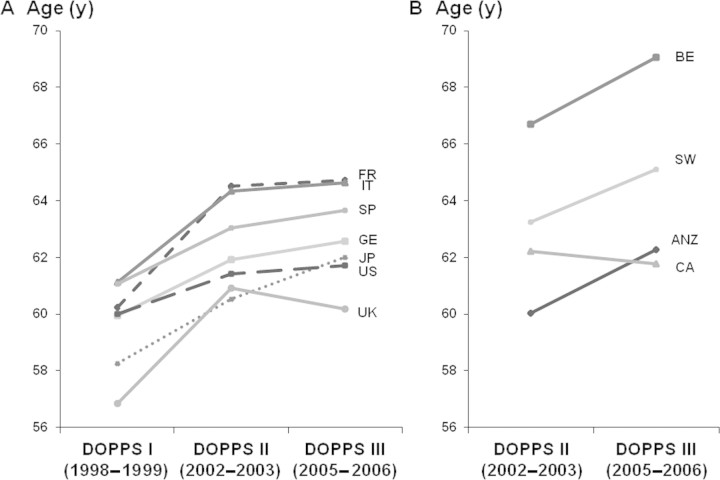
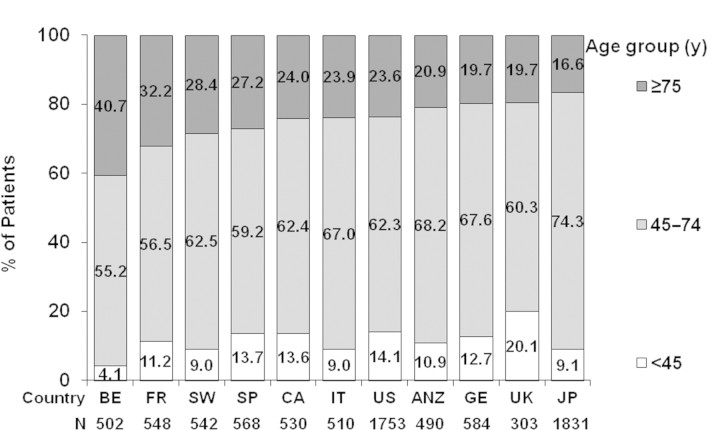
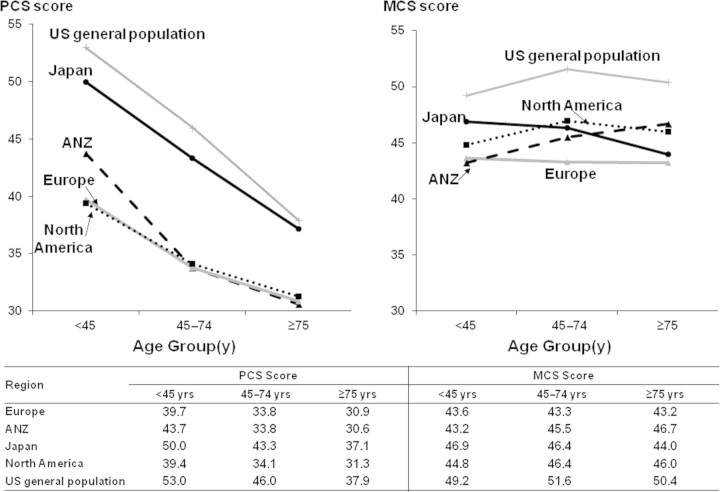
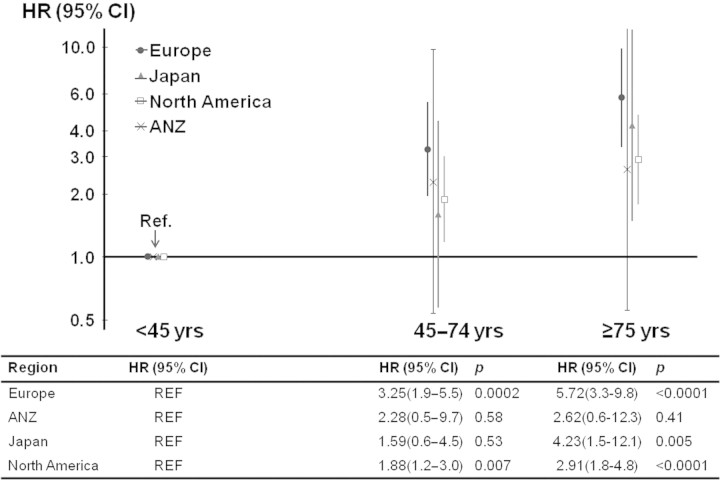
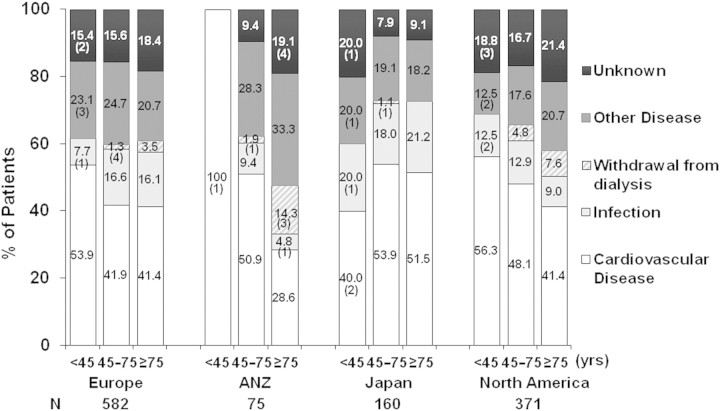
Results: Although participant mean age increased over time in all DOPPS countries, the percentage of elderly varied widely. Overall, comorbidities and malnutrition were more common in the elderly. Fistulae were used less frequently among elderly versus younger patients in Europe and North America but not in Australia, New Zealand, and Japan. No difference in treatment time was observed between elderly and younger patients after normalizing for body weight. In all regions, ultrafiltration rates were lower among elderly patients. Elderly patients reported poorer quality of life with respect to the physical but not mental component scores. Mortality risk was three- to sixfold higher in the elderly group, whereas causes of death overall were similar for elderly and younger patients.
Conclusions: Elderly patients represent a different proportion of DOPPS participants across countries, possibly reflecting differences in policies and clinical practices. In general, hemodialysis practices in the elderly reflected each region's clinical patterns, with some variation by age group depending upon the practice.
Figures

References
-
- Collins AJ, Kasiske B, Herzog C, Chavers B, Foley R, Gilbertson D, Grimm R, Liu J, Louis T, Manning W, McBean M, Murray A, St Peter W, Xue J, Fan Q, Guo H, Li Q, Li S, Qiu Y, Li S, Roberts T, Skeans M, Snyder J, Solid C, Wang C, Weinhandl E, Zhang R, Arko C, Chen SC, Dalleska F, Daniels F, Dunning S, Ebben J, Frazier E, Hanzlik C, Johnson R, Sheets D, Wang X, Forrest B, Berrini D, Constantini E, Everson S, Eggers P, Agodoa L: Excerpts from the United States Renal Data System 2006 Annual Data Report. Am J Kidney Dis 49 [Suppl]: A6–A7, S1–S296, 2007 - PubMed
-
- Jager KJ, van Dijk PC, Dekker FW, Stengel B, Simpson K, Briggs JD: The epidemic of aging in renal replacement therapy: An update on elderly patients and their outcomes. Clin Nephrol 60: 352–360, 2003 - PubMed
-
- Kurella M, Covinsky KE, Collins AJ, Chertow GM: Octogenarians and nonagenarians starting dialysis in the United States. Ann Intern Med 146: 177–183, 2007 - PubMed
-
- ERA-EDTA Registry: ERA-EDTA Registry 2005 Annual Report. Amsterdam, The Netherlands, Academic Medical Center, Department of Medical Informatics, June 2007
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
