

Increasing incidence of Ehrlichia chaffeensis and Anaplasma phagocytophilum in the United States, 2000-2007
- PMID: 21734137
- PMCID: PMC3122356
- DOI: 10.4269/ajtmh.2011.10-0613
Increasing incidence of Ehrlichia chaffeensis and Anaplasma phagocytophilum in the United States, 2000-2007
Abstract
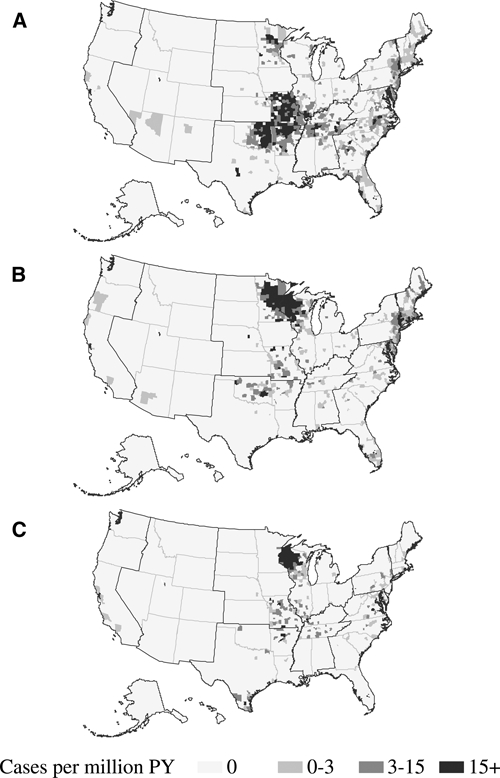
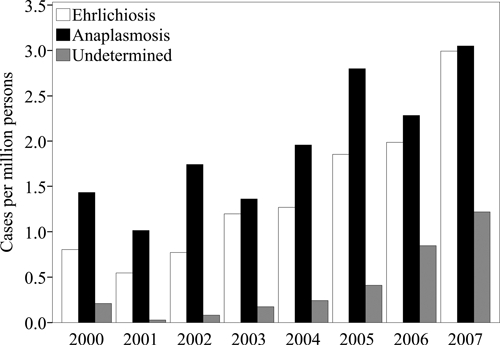
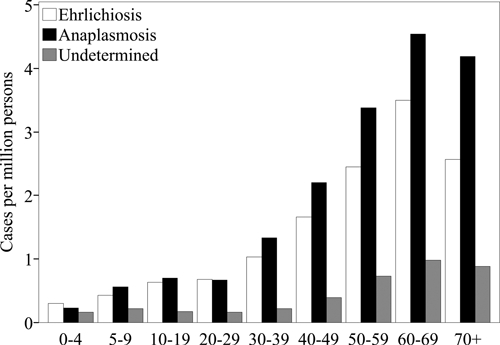
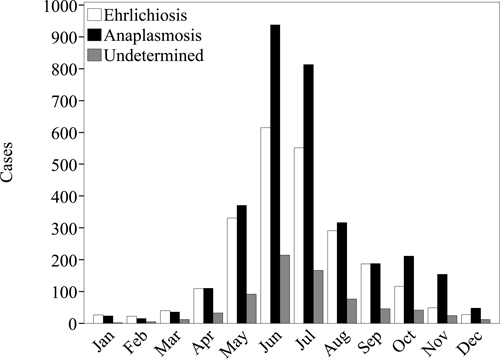
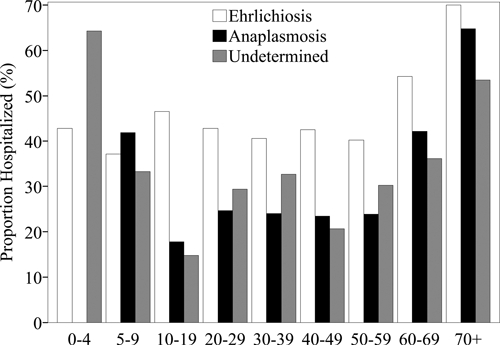
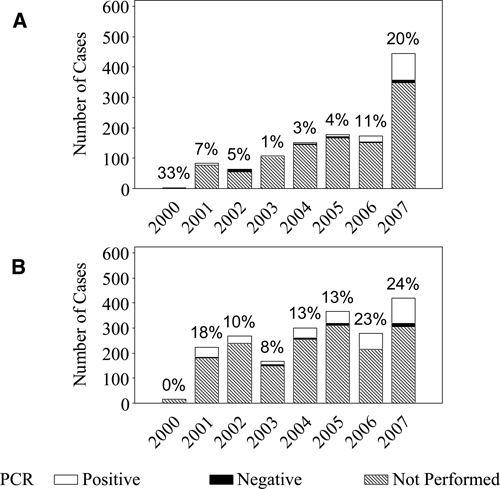
Ehrlichia chaffeensis causes human monocytic ehrlichiosis, and Anaplasma phagocytophilum causes human granulocytic anaplasmosis. These related tick-borne rickettsial organisms can cause severe and fatal illness. During 2000-2007, the reported incidence rate of E. chaffeensis increased from 0.80 to 3.0 cases/million persons/year. The case-fatality rate was 1.9%, and the hospitalization rate was 49%. During 2000-2007, the reported incidence of A. phagocytophilum increased from 1.4 to 3.0 cases/million persons/year. The case-fatality rate was 0.6%, and the hospitalization rate was 36%. Rates among female patients were lower than among male patients for ehrlichiosis (rate ratio = 0.68) and anaplasmosis (rate ratio = 0.70). Most (80%) ehrlichiosis and anaplasmosis cases met only a probable case definition, although, use of a polymerase chain reaction to confirm infections increased during 2000-2007. Heightened reporting of these diseases will likely continue with improving recognition, changing surveillance practices, and appropriate application of diagnostic assays.
Figures
References
-
- Maeda K, Markowitz N, Hawley RC, Ristic M, Cox D, Mcdade JE. Human infection with Ehrlichia canis, a leukocytic Rickettsia. N Engl J Med. 1987;316:853–856. - PubMed
-
- Dumler JS, Bakken JS, Eckman MR, Vanetta LL, Chen SM, Walker DH. Human granulocytic ehrlichiosis: a new, potentially fatal tick-borne infection diagnosed by peripheral blood smear and PCR. Lab Invest. 1994;70:A126–A126.
-
- Bakken JS, Dumler JS, Chen SM, Eckman MR, Vanetta LL, Walker DH. Human granulocytic ehrlichiosis in the upper midwest United States: a new species emerging? JAMA. 1994;272:212–218. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
