

Real-time FDG PET guidance during biopsies and radiofrequency ablation using multimodality fusion with electromagnetic navigation
- PMID: 21734159
- PMCID: PMC3157001
- DOI: 10.1148/radiol.11101985
Real-time FDG PET guidance during biopsies and radiofrequency ablation using multimodality fusion with electromagnetic navigation
Abstract
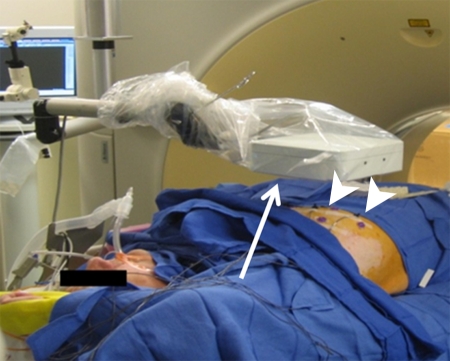
Purpose: To assess the feasibility of combined electromagnetic device tracking and computed tomography (CT)/ultrasonography (US)/fluorine 18 fluorodeoxyglucose (FDG) positron emission tomography (PET) fusion for real-time feedback during percutaneous and intraoperative biopsies and hepatic radiofrequency (RF) ablation.
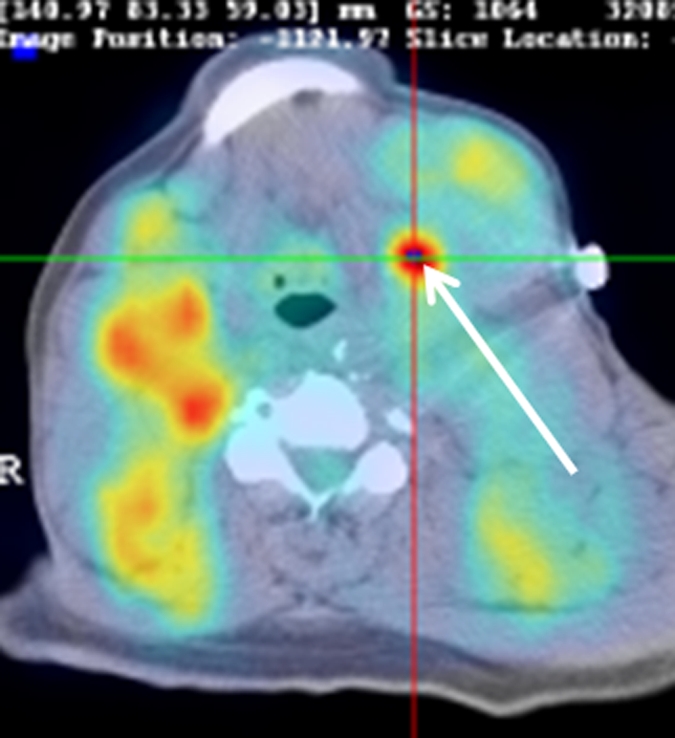
Materials and methods: In this HIPAA-compliant, institutional review board-approved prospective study with written informed consent, 25 patients (17 men, eight women) underwent 33 percutaneous and three intraoperative biopsies of 36 FDG-avid targets between November 2007 and August 2010. One patient underwent biopsy and RF ablation of an FDG-avid hepatic focus. Targets demonstrated heterogeneous FDG uptake or were not well seen or were totally inapparent at conventional imaging. Preprocedural FDG PET scans were rigidly registered through a semiautomatic method to intraprocedural CT scans. Coaxial biopsy needle introducer tips and RF ablation electrode guider needle tips containing electromagnetic sensor coils were spatially tracked through an electromagnetic field generator. Real-time US scans were registered through a fiducial-based method, allowing US scans to be fused with intraprocedural CT and preacquired FDG PET scans. A visual display of US/CT image fusion with overlaid coregistered FDG PET targets was used for guidance; navigation software enabled real-time biopsy needle and needle electrode navigation and feedback.
Results: Successful fusion of real-time US to coregistered CT and FDG PET scans was achieved in all patients. Thirty-one of 36 biopsies were diagnostic (malignancy in 18 cases, benign processes in 13 cases). RF ablation resulted in resolution of targeted FDG avidity, with no local treatment failure during short follow-up (56 days).
Conclusion: Combined electromagnetic device tracking and image fusion with real-time feedback may facilitate biopsies and ablations of focal FDG PET abnormalities that would be challenging with conventional image guidance.
Figures









References
-
- Czernin J, Benz MR, Allen-Auerbach MS. PET/CT imaging: The incremental value of assessing the glucose metabolic phenotype and the structure of cancers in a single examination. Eur J Radiol 2010;73(3):470–480 - PubMed
-
- Poeppel TD, Krause BJ, Heusner TA, Boy C, Bockisch A, Antoch G. PET/CT for the staging and follow-up of patients with malignancies. Eur J Radiol 2009;70(3):382–392 - PubMed
-
- Ahmadzadehfar H, Rodrigues M, Zakavi R, Knoll P, Mirzaei S. Prognostic significance of the standardized uptake value of pre-therapeutic 18F-FDG PET in patients with malignant lymphoma. Med Oncol. doi:10.1007/s12032-010-9584-2. Published June 4, 2010. Accessed May 25, 2011 - PubMed
-
- Arulampalam TH, Costa DC, Loizidou M, Visvikis D, Ell PJ, Taylor I. Positron emission tomography and colorectal cancer. Br J Surg 2001;88(2):176–189 - PubMed
-
- Berghmans T, Dusart M, Paesmans M, et al. Primary tumor standardized uptake value (SUVmax) measured on fluorodeoxyglucose positron emission tomography (FDG-PET) is of prognostic value for survival in non-small cell lung cancer (NSCLC): a systematic review and meta-analysis (MA) by the European Lung Cancer Working Party for the IASLC Lung Cancer Staging Project. J Thorac Oncol 2008;3(1):6–12 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
