

Antidepressants for the treatment of abdominal pain-related functional gastrointestinal disorders in children and adolescents
- PMID: 21735420
- PMCID: PMC6769179
- DOI: 10.1002/14651858.CD008013.pub2
Antidepressants for the treatment of abdominal pain-related functional gastrointestinal disorders in children and adolescents
Update in
-
Antidepressants for functional abdominal pain disorders in children and adolescents.Cochrane Database Syst Rev. 2021 Feb 9;2(2):CD008013. doi: 10.1002/14651858.CD008013.pub3. Cochrane Database Syst Rev. 2021. PMID: 33560523 Free PMC article.
Abstract
Background: Abdominal pain-related functional gastrointestinal disorders (FGIDs) are among the most common medical problems in paediatric medicine. Frequently, physicians prescribe antidepressants as a second-line treatment for children and adolescents with FGIDs. To date, the evidence on the benefits and harms of antidepressants for the treatment of abdominal pain-related FGIDs has not been assessed systematically.
Objectives: The primary objectives were to conduct a systematic review to evaluate the efficacy and safety of antidepressants for the treatment of abdominal pain-related FGIDs in children and adolescents.
Search strategy: We searched The Cochrane Library, PubMed, EMBASE, IPA, CINAHL, PsycINFO, ISI Web of Science, Biosis Previews and the International Clinical Trials Registry Platform of the World Health Organization with appropriate filters (from inception to January 31, 2011).
Selection criteria: For efficacy we included double-blind, randomised controlled trials (RCTs) of antidepressants for treatment of abdominal pain-related FGIDs in children and adolescents 18 years or younger. Open-label and uncontrolled experimental studies, as well as observational studies were eligible for the assessment of harms. The minimum study duration was 4 weeks. The minimum study size was 30 participants.
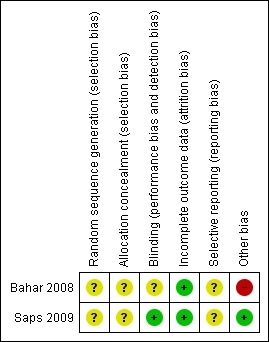
Data collection and analysis: Two authors independently assessed all abstracts and full text articles, and rated the risk of bias for included studies. Data were extracted independently by one author and checked for accuracy by another author. Data were analysed using RevMan 5.
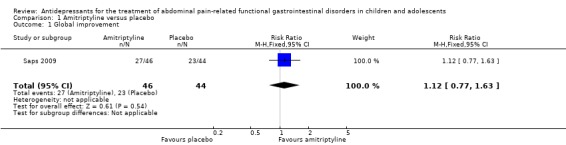
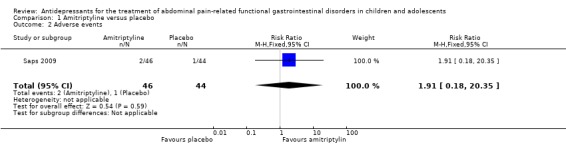
Main results: Two RCTs (123 participants), both using amitriptyline, met the pre-specified inclusion criteria. These studies provided mixed findings on the efficacy of amitriptyline for the treatment of abdominal pain-related FGIDs. The larger, publicly-funded study reported no statistically significant difference in efficacy between amitriptyline and placebo in 90 children and adolescents with FGIDs after 4 weeks of treatment. On intention-to-treat (ITT)- analysis, 59% of the children reported feeling better in the amitriptyline group compared with 53% in the placebo group (RR 1.12; 95% CI: 0.77 to 1.63; P = 0.54). The risk of bias for this study was rated as low.The second RCT enrolled 33 adolescents with irritable bowel syndrome. Patients receiving amitriptyline experienced greater improvements in the primary outcome, overall quality of life, at weeks 6, 10, and 13 compared with those on placebo (P= 0.019, 0.004, and 0.013, respectively). No effect estimates were calculated for the quality of life outcome because mean quality of life scores and standard deviations were not reported. For most secondary outcomes no statistically significant differences between amitriptyline and placebo could be detected. The risk of bias for this study was rated as unclear for most items. However, it was rated as high for other bias due to multiple testing. The results of this study should be interpreted with caution due to the small number of patients and multiple testing.The larger study reported mild adverse events including fatigue, rash and headache and dizziness. On ITT analysis, 4% of the amitriptyline group experienced at least one adverse event compared to 2% of the placebo group. There was no statistically significant difference in the proportion of patients who experienced at least one adverse event (RR 1.91; 95% CI 0.18 to 20.35; P = 0.59). The smaller study reported no adverse events. The methods of adverse effects assessment was poorly reported in both studies and no clear conclusions on the risks of harms of amitriptyline can be drawn.
Authors' conclusions: Clinicians must be aware that for the majority of antidepressant medications no evidence exists that supports their use for the treatment of abdominal pain-related FGIDs in children and adolescents. The existing randomised controlled evidence is limited to studies on amitriptyline and revealed no statistically significant differences between amitriptyline and placebo for most efficacy outcomes. Amitriptyline does not appear to provide any benefit for the treatment of FGIDs in children and adolescents. Studies in children with depressive disorders have shown that antidepressants can lead to substantial, sometimes life-threatening adverse effects. Until better evidence evolves, clinicians should weigh the potential benefits of antidepressant treatment against known risks of antidepressants in paediatric patients.
Conflict of interest statement
None known.
Figures
Similar articles
-
Antidepressants for chronic non-cancer pain in children and adolescents.Cochrane Database Syst Rev. 2017 Aug 5;8(8):CD012535. doi: 10.1002/14651858.CD012535.pub2. Cochrane Database Syst Rev. 2017. PMID: 28779487 Free PMC article.
-
Antiepileptic drugs for chronic non-cancer pain in children and adolescents.Cochrane Database Syst Rev. 2017 Aug 5;8(8):CD012536. doi: 10.1002/14651858.CD012536.pub2. Cochrane Database Syst Rev. 2017. PMID: 28779491 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Amitriptyline for neuropathic pain and fibromyalgia in adults.Cochrane Database Syst Rev. 2012 Dec 12;12:CD008242. doi: 10.1002/14651858.CD008242.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 Jul 06;(7):CD008242. doi: 10.1002/14651858.CD008242.pub3. PMID: 23235657 Updated.
Cited by
-
Chinese Herbal Medicine for Functional Abdominal Pain Syndrome: From Clinical Findings to Basic Understandings.Evid Based Complement Alternat Med. 2016;2016:8652523. doi: 10.1155/2016/8652523. Epub 2016 Jun 5. Evid Based Complement Alternat Med. 2016. PMID: 27366194 Free PMC article. Review.
-
Drugs for chronic pain in children: a commentary on clinical practice and the absence of evidence.Pain Res Manag. 2013 Jan-Feb;18(1):47-50. doi: 10.1155/2013/402863. Pain Res Manag. 2013. PMID: 23457686 Free PMC article. Review.
-
Viral and atypical respiratory co-infections in COVID-19: a systematic review and meta-analysis.J Am Coll Emerg Physicians Open. 2020 Jun 19;1(4):533-548. doi: 10.1002/emp2.12128. eCollection 2020 Aug. J Am Coll Emerg Physicians Open. 2020. PMID: 32838380 Free PMC article.
-
Antidepressants for functional gastrointestinal disorders in children.Can Fam Physician. 2013 Mar;59(3):263-4. Can Fam Physician. 2013. PMID: 23486795 Free PMC article.
-
Pain management in patients with inflammatory bowel disease: insights for the clinician.Therap Adv Gastroenterol. 2012 Sep;5(5):339-57. doi: 10.1177/1756283X12446158. Therap Adv Gastroenterol. 2012. PMID: 22973418 Free PMC article.
References
References to studies included in this review
-
- Bahar RJ, Collins BS, Steinmetz B, Ament ME. Double‐blind placebo‐controlled trial of amitriptyline for the treatment of irritable bowel syndrome in adolescents. J Pediatr 2008;152(2):685‐9. [PUBMED: 18410774] - PubMed
References to studies excluded from this review
-
- Campo JV, Perel J, Lucas A, Bridge J, Ehmann M, Kalas C, et al. Citalopram treatment of pediatric recurrent abdominal pain and comorbid internalizing disorders: an exploratory study. J Am Acad Child Adolesc Psychiatry 2004;43(10):1234‐42. [PUBMED: 15381890] - PubMed
References to ongoing studies
-
- Anxiety and Recurrent Abdominal Pain in Children. Ongoing study July 2004 to April 2010.
Additional references
-
- Anonymous. Report of the CSM expert working group on the safety of selective serotonin reuptake inhibitor antidepressants. Medicines and Healthcare Products Regulatory Agency2004, issue http://www.mhra.gov.uk/home/groups/pl‐p/documents/drugsafetymessage/con0....
-
- Brandt LJ, Chey WD, Foxx‐Orenstein AE, Schiller LR, Schoenfeld PS, Spiegel BM, et al. An evidence‐based position statement on the management of irritable bowel syndrome. Am J Gastroenterol 2009;104 Suppl 1:S1‐35. [PUBMED: 19521341] - PubMed
-
- Chitkara DK, Rawat DJ, Talley NJ. The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. Am J Gastroenterol 2005;100(8):1868‐75. [PUBMED: 16086724] - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous