

Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction
- PMID: 21737017
- PMCID: PMC3272542
- DOI: 10.1016/j.jacc.2011.02.055
Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction
Abstract
Objectives: The purpose of this study was to determine the mechanisms responsible for reduced aerobic capacity (peak Vo(2)) in patients with heart failure with preserved ejection fraction (HFPEF).
Background: HFPEF is the predominant form of heart failure in older persons. Exercise intolerance is the primary symptom among patients with HFPEF and a major determinant of reduced quality of life. In contrast to patients with heart failure and reduced ejection fraction, the mechanism of exercise intolerance in HFPEF is less well understood.
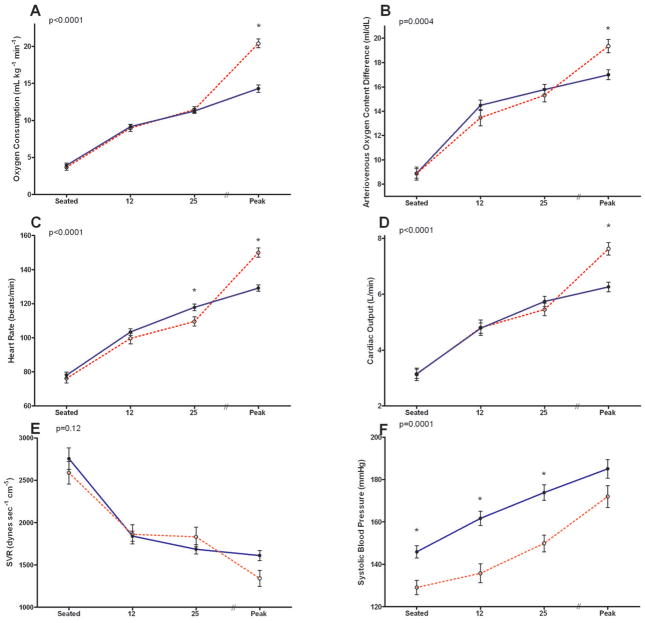
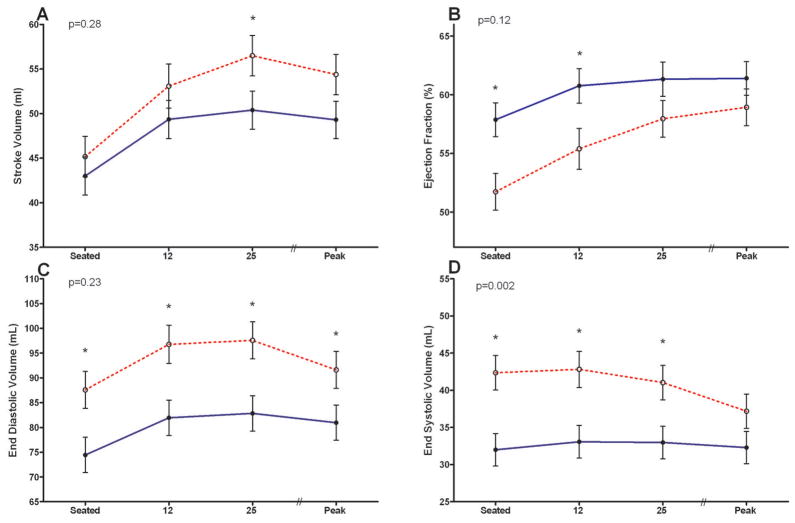
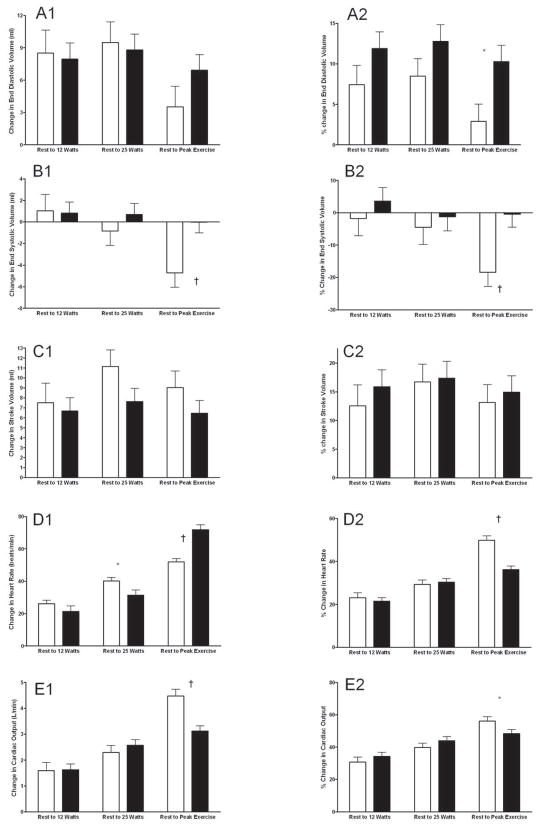
Methods: Left ventricular volumes (2-dimensional echocardiography), cardiac output, Vo(2), and calculated arterial-venous oxygen content difference (A-Vo(2) Diff) were measured at rest and during incremental, exhaustive upright cycle exercise in 48 HFPEF patients (age 69 ± 6 years) and 25 healthy age-matched controls.
Results: In HFPEF patients compared with healthy controls, Vo(2) was reduced at peak exercise (14.3 ± 0.5 ml·kg·min(-1) vs. 20.4 ± 0.6 ml·kg·min(-1); p < 0.0001) and was associated with a reduced peak cardiac output (6.3 ± 0.2 l·min(-1) vs. 7.6 ± 0.2 l·min(-1); p < 0.0001) and A-Vo(2) Diff (17 ± 0.4 ml·dl(-1) vs. 19 ± 0.4 ml·dl(-1), p < 0.0007). The strongest independent predictor of peak Vo(2) was the change in A-Vo(2) Diff from rest to peak exercise (A-Vo(2) Diff reserve) for both HFPEF patients (partial correlate, 0.58; standardized β coefficient, 0.66; p = 0.0002) and healthy controls (partial correlate, 0.61; standardized β coefficient, 0.41; p = 0.005).
Conclusions: Both reduced cardiac output and A-Vo(2) Diff contribute significantly to the severe exercise intolerance in elderly HFPEF patients. The finding that A-Vo(2) Diff reserve is an independent predictor of peak Vo(2) suggests that peripheral, noncardiac factors are important contributors to exercise intolerance in these patients.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Potential conflicts of interest: Dr. Kitzman is a consultant for Relypsa Inc, and Boston Scientific Corp. He has received grant support from Novartis and Bristol-Meyers-Squibb. The authors have no other conflicts of interest to report.
Figures
Comment in
-
Heart failure with a preserved ejection fraction: what is in a name?J Am Coll Cardiol. 2011 Jul 12;58(3):275-7. doi: 10.1016/j.jacc.2011.02.054. J Am Coll Cardiol. 2011. PMID: 21737018 No abstract available.
-
Determinants of exercise intolerance in heart failure with preserved ejection fraction.J Am Coll Cardiol. 2011 Dec 6;58(24):2547-8; author reply 2548-9. doi: 10.1016/j.jacc.2011.08.048. J Am Coll Cardiol. 2011. PMID: 22133861 No abstract available.
References
-
- Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the community: a study of all incident cases in Olmsted County, Minnesota, in 1991. Circulation. 1998;98:2282–9. - PubMed
-
- Kitzman DW, Gardin JM, Gottdiener JS, et al. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. CHS Research Group. Cardiovascular Health Study. Am J Cardiol. 2001;87:413–9. - PubMed
-
- Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. J Am Coll Cardiol. 1999;33:1948–55. - PubMed
-
- Kitzman DW, Little WC, Brubaker PH, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. Jama. 2002;288:2144–50. - PubMed
-
- Wilson JR, Mancini DM, Dunkman WB. Exertional fatigue due to skeletal muscle dysfunction in patients with heart failure. Circulation. 1993;87:470–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
