

Phenotypic spectrum and management of sternal cleft: literature review and presentation of a new series
- PMID: 21737294
- PMCID: PMC3241094
- DOI: 10.1016/j.ejcts.2011.05.049
Phenotypic spectrum and management of sternal cleft: literature review and presentation of a new series
Abstract
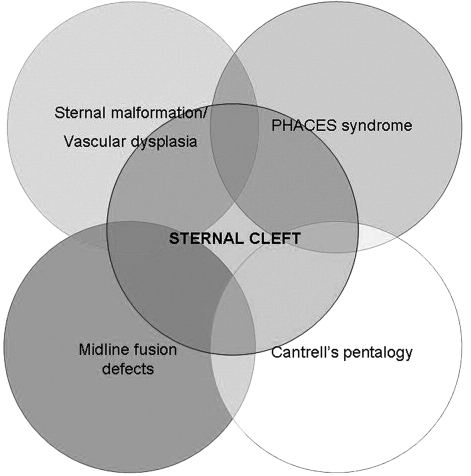
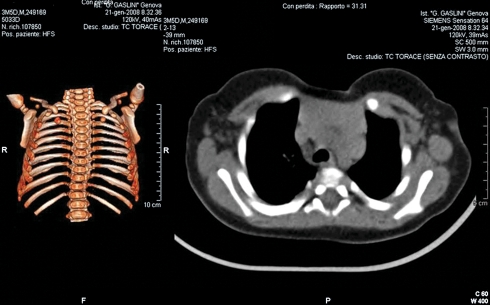
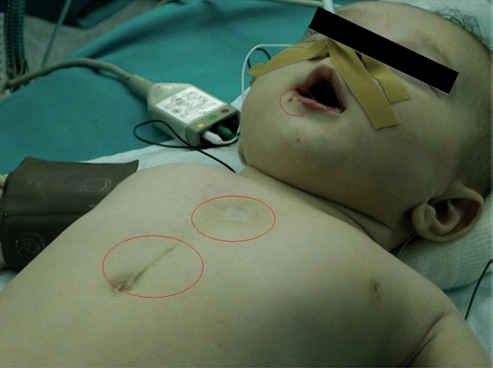
Sternal cleft is a chest wall malformation that can expose mediastinal viscera and vessels to injuries. It can be classified into two forms, complete and partial. Its etiology and incidence are unknown and it is often associated with other defects. The aim of this article is to review the literature and report our experience with this rare anomaly, focusing on clinical presentation and management. We reviewed the English written literature about sternal cleft and collected the clinical data of all the published series. We present seven new cases that we have observed and treated since 1999. Literature reports 51 series including 86 patients, more frequently female (62%) and affected with partial superior form (67%). Sternal cleft is often asymptomatic (74%) and associated with other defects (72%). Surgical treatments include primary closure (73%), bone graft interposition (10%), prosthetic closure (7%), and muscle flap interposition (3%). In our series, primary closure was possible in four cases, while in three cases we placed a prosthesis. Five patients had associated defects and two were affected with PHACES (posterior fossa abnormalities, hemangiomas, arterial lesions, cardiac abnormalities/aortic coarctation, abnormalities of the eye, and sternum defects) syndrome. We report for the first time the association of sternal cleft with connectival nevi in three of our patients. At follow-up, we observed no major complication or recurrences. Although primary closure is the preferred option and should be performed in the neonatal period, the use of prostheses warrants good results as well. Prior to treatment, associated defects and syndromes should be excluded.
Figures


References
-
- Engum SA. Embryology sternal clefts, ectopia cordis, and Cantrell’s pentalogy. Semin Pediatr Surg. 2008:154–60. - PubMed
-
- Acastello E, Majluf R, Garrido P, Barbosa LM, Peredo A. Sternal cleft: a surgical opportunity. J Pediatr Surg. 2003:178–83. - PubMed
-
- Forzano F, Daubeney PE, White SM. Midline raphe, sternal cleft, and other midline abnormalities: a new dominant syndrome? Am J Med Genet A. 2005;135:9–12. - PubMed
-
- Daum R, Zachariou Z. Total and superior sternal clefts in newborns: a simple technique for surgical correction. J Pediatr Surg. 1999:408–11. - PubMed
-
- Domini M, Cupaioli M, Rossi F, Fakhro A, Aquino A, Chiesa PL. Bifid sternum: neonatal surgical treatment. Ann Thorac Surg. 2000:267–9. - PubMed
