

Immunosuppression in patients with high-grade gliomas treated with radiation and temozolomide
- PMID: 21737504
- PMCID: PMC3156964
- DOI: 10.1158/1078-0432.CCR-11-0774
Immunosuppression in patients with high-grade gliomas treated with radiation and temozolomide
Abstract
Purpose: Patients with high-grade gliomas (HGG) routinely receive radiation, temozolomide, and glucocorticoids. As each of these is immunosuppressive, we conducted a prospective, multicenter study to follow CD4 counts over time and determine whether low CD4 counts were associated with adverse outcomes.
Experimental design: Patients with newly diagnosed HGG had CD4 counts drawn before initiating standard therapy and monthly thereafter for 1 year. Information on hospitalizations, infections, glucocorticoid use, survival, and cause of death were also collected.
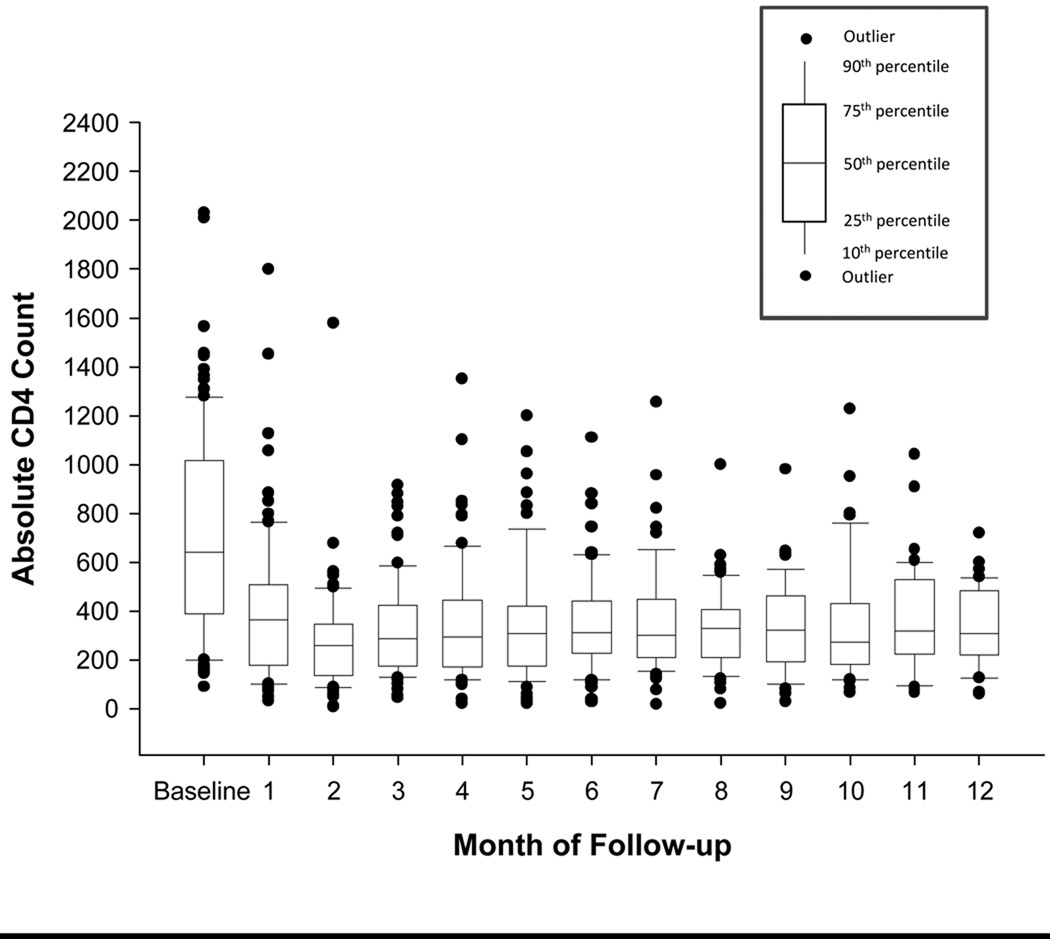
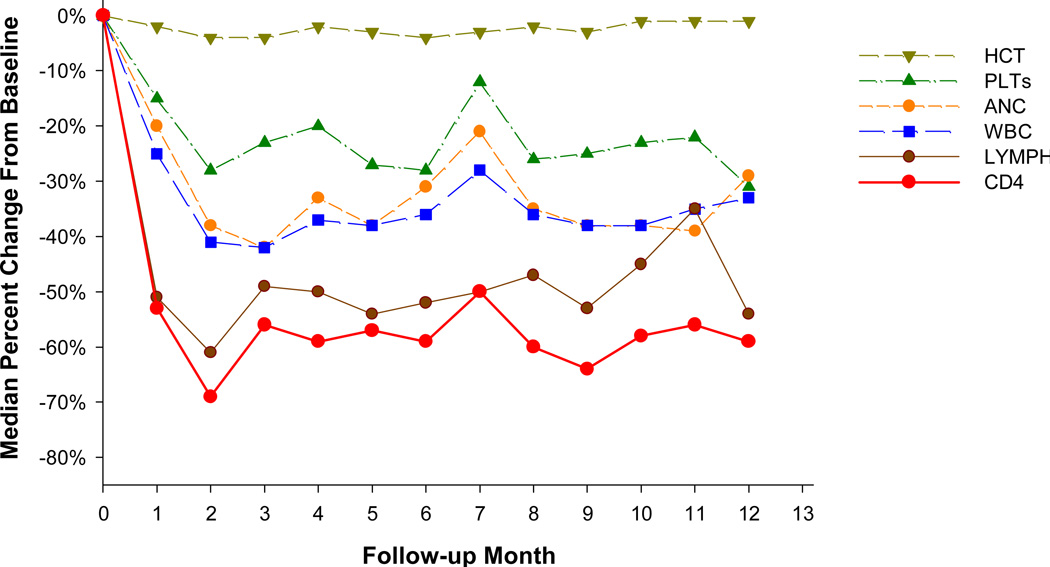
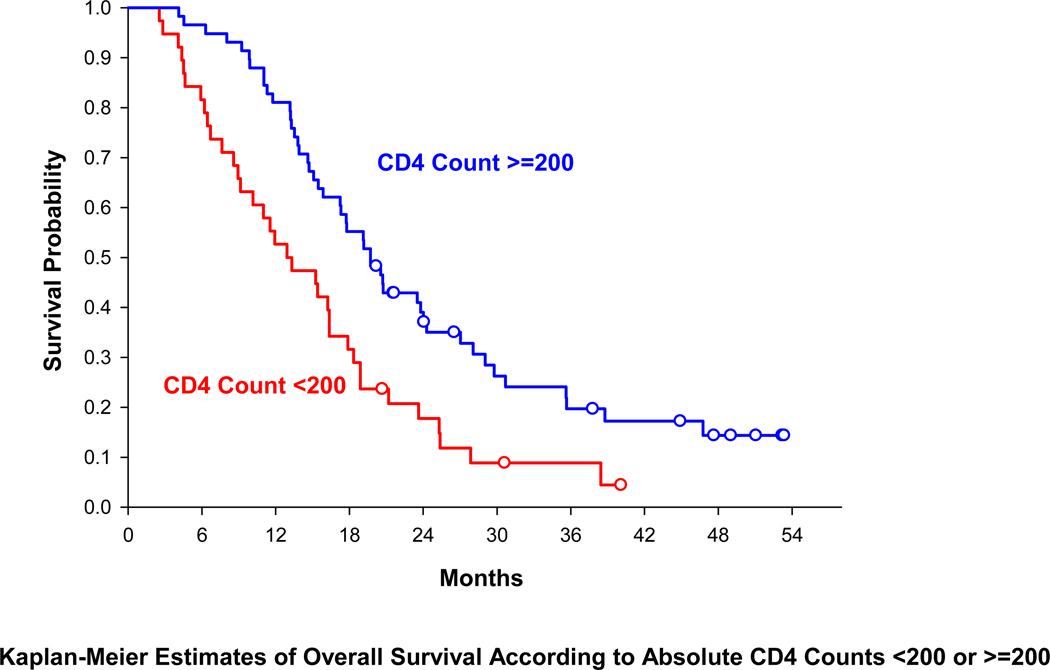
Results: Ninety-six evaluable patients were accrued [85% glioblastoma, median age of 57, median Karnofsky performance status (KPS) = 90]. The median CD4 count before radiation and temozolomide treatment was 664 cells/mm(3). The CD4 count nadir occurred 2 months after initiating therapy when 73% of patients had CD4 counts less than 300 cells/mm(3) and 40% had less than 200 cells/mm(3). CD4 counts remained low throughout the year of follow-up. Patients with CD4 counts less than 200 cells/mm(3)at 2 months had shorter survival than those with higher counts (median: 13.1 vs. 19.7 months, P = 0.002). Median survival was related to CD4 toxicity grades (I = 23.8 months, II = 19.7 months, III-IV = 13.1 months, P = 0.009). The adjusted HR for death attributable to 2-month CD4 count below 200 was 1.66 (P = 0.03). Eighty-eight percent of deaths resulted from disease progression, whereas only 2.5% were due to infection.
Conclusions: Severe reductions in CD4 counts in patients with newly diagnosed HGG treated with radiation and temozolomide treatment are common, treatment-related, long-lasting, and associated with early death from tumor progression.
©2011 AACR.
Conflict of interest statement
Figures
References
-
- Masur H. Prevention and treatment of pneumocystis pneumonia. N Engl J Med. 1992;327(26):1853–1860. - PubMed
-
- Masur H, Lane HC, Kovacs JA, Allegra CJ, Edman JC. NIH conference. pneumocystis pneumonia: From bench to clinic; Ann Intern Med; 1989. pp. 813–826. - PubMed
-
- Arend SM, Kroon FP, van't Wout JW. Pneumocystis carinii pneumonia in patients without AIDS, 1980 through 1993. an analysis of 78 cases. Arch Intern Med. 1995;155(22):2436–2441. - PubMed
-
- Browne MJ, Hubbard SM, Longo DL, Fisher R, Wesley R, Ihde DC, et al. Excess prevalence of pneumocystis carinii pneumonia in patients treated for lymphoma with combination chemotherapy. Ann Intern Med. 1986;104(3):338–344. - PubMed
-
- Gluck T, Geerdes-Fenge HF, Straub RH, Raffenberg M, Lang B, Lode H, et al. Pneumocystis carinii pneumonia as a complication of immunosuppressive therapy. Infection. 2000;28(4):227–230. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
