

Cardiac complications in patients with community-acquired pneumonia: a systematic review and meta-analysis of observational studies
- PMID: 21738449
- PMCID: PMC3125176
- DOI: 10.1371/journal.pmed.1001048
Cardiac complications in patients with community-acquired pneumonia: a systematic review and meta-analysis of observational studies
Abstract
Background: Community-acquired pneumonia (CAP) is a leading cause of morbidity and mortality. CAP can trigger acute cardiac events. We sought to determine the incidence of major cardiac complications in CAP patients to characterize the magnitude of this problem.
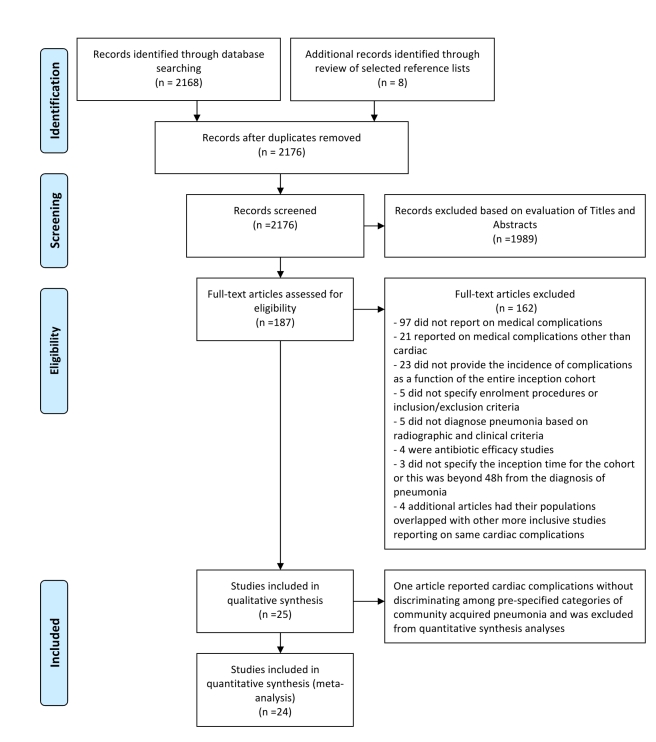
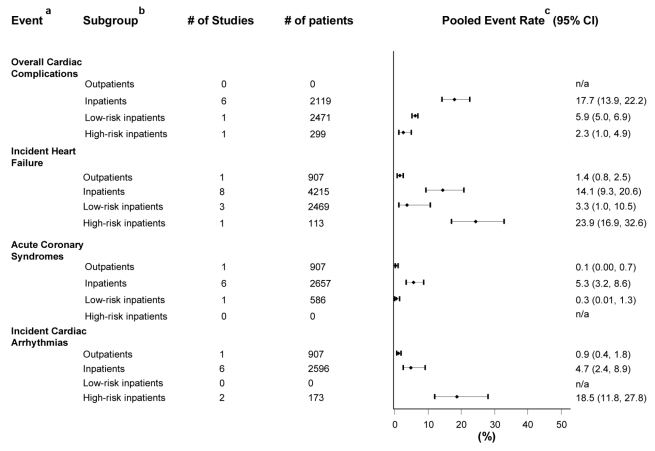
Methods and findings: Two investigators searched MEDLINE, Scopus, and EMBASE for observational studies of immunocompetent adults with clinical and radiological evidence of CAP that reported any of the following: overall cardiac complications, incident heart failure, acute coronary syndromes (ACS), or incident cardiac arrhythmias occurring within 30 days of CAP diagnosis. At a minimum, studies had to establish enrolment procedures and inclusion and exclusion criteria, enroll their patients sequentially, and report the incidence of cardiac complications as a function of their entire cohorts. Studies with focus on nosocomial or health care-associated pneumonia were not included. Review of 2,176 citations yielded 25 articles that met eligibility and minimum quality criteria. Seventeen articles (68%) reported cohorts of CAP inpatients. In this group, the pooled incidence rates for overall cardiac complications (six cohorts, 2,119 patients), incident heart failure (eight cohorts, 4,215 patients), acute coronary syndromes (six cohorts, 2,657 patients), and incident cardiac arrhythmias (six cohorts, 2,596 patients), were 17.7% (confidence interval [CI] 13.9-22.2), 14.1% (9.3-20.6), 5.3% (3.2-8.6), and 4.7% (2.4-8.9), respectively. One article reported cardiac complications in CAP outpatients, four in low-risk (not severely ill) inpatients, and three in high-risk inpatients. The incidences for all outcomes except overall cardiac complications were lower in the two former groups and higher in the latter. One additional study reported on CAP outpatients and low-risk inpatients without discriminating between these groups. Twelve studies (48%) asserted the evaluation of cardiac complications in their methods but only six (24%) provided a definition for them. Only three studies, all examining ACS, carried out risk factor analysis for these events. No study analyzed the association between cardiac complications and other medical complications or their impact on other CAP outcomes.
Conclusions: Major cardiac complications occur in a substantial proportion of patients with CAP. Physicians and patients need to appreciate the significance of this association for timely recognition and management of these events. Strategies aimed at preventing pneumonia (i.e., influenza and pneumococcal vaccination) in high-risk populations need to be optimized. Further research is needed to understand the mechanisms underlying this association, measure the impact of cardiac complications on other CAP outcomes, identify those patients with CAP at high risk of developing cardiac complications, and design strategies to prevent their occurrence in this population.
Conflict of interest statement
VFCM has provided consulting services to CEMPRA pharmaceuticals. GR is involved in a research study sponsored by CEMPRA pharmaceuticals.
Figures
References
-
- Raut M, Schein J, Mody S, Grant R, Benson C, et al. Estimating the economic impact of a half-day reduction in length of hospital stay among patients with community-acquired pneumonia in the US. Curr Med Res Opin. 2009;25:2151–2157. - PubMed
-
- File TM, Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122:130–141. - PubMed
-
- Fry AM, Shay DK, Holman RC, Curns AT, Anderson LJ. Trends in hospitalizations for pneumonia among persons aged 65 years or older in the United States, 1988–2002. JAMA. 2005;294:2712–2719. - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. Heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- United States Census Bureau. 2008 National Population Projections. Washington (D.C.): U.S. Census Bureau;
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
