

Subcorneal pustular dermatosis an immnohisto-pathological perspective
- PMID: 21738824
- PMCID: PMC3127074
Subcorneal pustular dermatosis an immnohisto-pathological perspective
Abstract
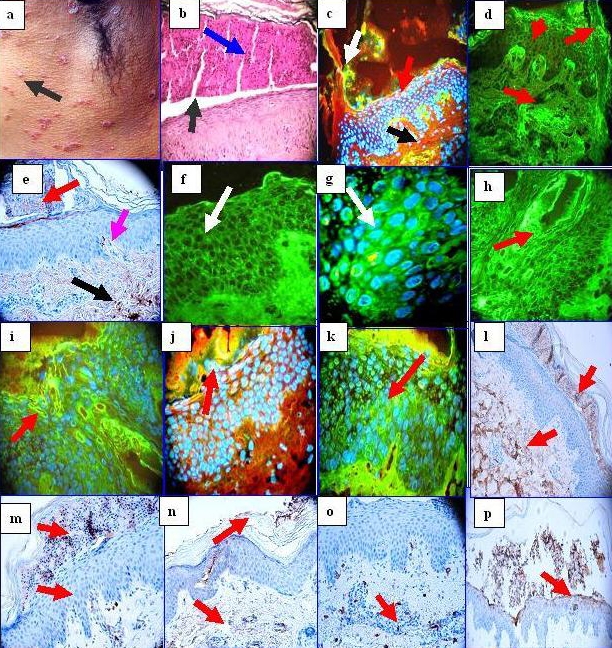
Subcorneal pustular dermatosis (SPD) represents a chronic, relapsing sterile pustular eruption, involving the trunk and flexoral proximal extremities. A 54-year-old female presented with recurrent, flaccid pustules measuring several millimeters in diameter, on normal and mildly erythematous skin of the groin and submammary areas. Biopsies for hematoxylin and eosin (H&E) examination, direct immunofluorescence (DIF) and immunohistochemistry (IHC) analysis were performed. The H&E staining demonstrated typical features of SPD, including some damage within dermal pilosebaceous units subjacent to the subcorneal blistering process. DIF revealed strong deposits of immunoreactants IgG, IgM, fibrinogen and complement/C3, present in a shaggy pattern within the subcorneal disease areas; in focal, areas of the basement membrane junction and in focal pericytoplasmic areas of epidermal keratinocytes. IHC revealed strong positivity to HLA-DPDQDR, mast cell tryptase, CD68, and ZAP-70 in the subcorneal inflammatory infiltrate, and surrounding dermal blood vessels. Myeloperoxidase was also positive. Positive staining with the anti-ribosomal protein S6-pS240 at the edges of hair follicles and sebaceous glands subjacent to the subcorneal blisters was also noted.
Conclusions: We conclude that this disorder may have several components in its etiopathology, including a possible restricted immune response and a possible genetic component; these possibilities warrant further investigation.
Keywords: HLA-DPDQDR; Subcorneal pustular dermatosis; ZAP-70; anti-ribosomal protein S6-pS240; mast cell tryptase.
Figures
References
-
- Sneddon IB, Wilkinson DS. Subcorneal pustular dermatoses. Br J Dermatol. 1956;68:385–394. - PubMed
-
- Nischal KC, Khopkar U. An approach to the diagnosis of neutrophilic dermatoses: A histo-pathological perspective. Indian J Dermatol Venereol Leprol. 2007;73:222–230. - PubMed
-
- Takata M, Inaoki M, Shodo M, Hirone T, Kaya H. Subcorneal pustular dermatosis associated with IgA myeloma and intraepidermal IgA deposits. Dermatology. 1994;189:111–114. - PubMed
-
- Scerri L, Zaki I, Allen BR. Pyoderma gangrenosum and subcorneal pustular dermatosis, without monoclonal gammopathy. Br J Dermatol. Mar. 1994;130:398–399. - PubMed
-
- Bordignon M, Zattra E, Montesco MC, Alaibac M. Subcorneal pustular dermatosis (Sneddon-Wilkinson disease) with absence of desmoglein 1 and 3 antibodies: case report and literature review. Am J Clin Dermatol. 2008;9:51–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous