

The effects of magnesium pretreatment on reperfusion injury during living donor liver transplantation
- PMID: 21738843
- PMCID: PMC3121087
- DOI: 10.4097/kjae.2011.60.6.408
The effects of magnesium pretreatment on reperfusion injury during living donor liver transplantation
Abstract
Background: Ischemia reperfusion (IR) injury is a complex phenomenon that leads to organ dysfunction and causes primary liver failure following liver transplantation. We investigated whether an intravenous administration of magnesium before reperfusion can prevent or reduce IR injury.
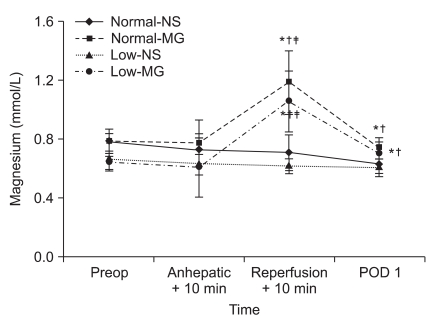
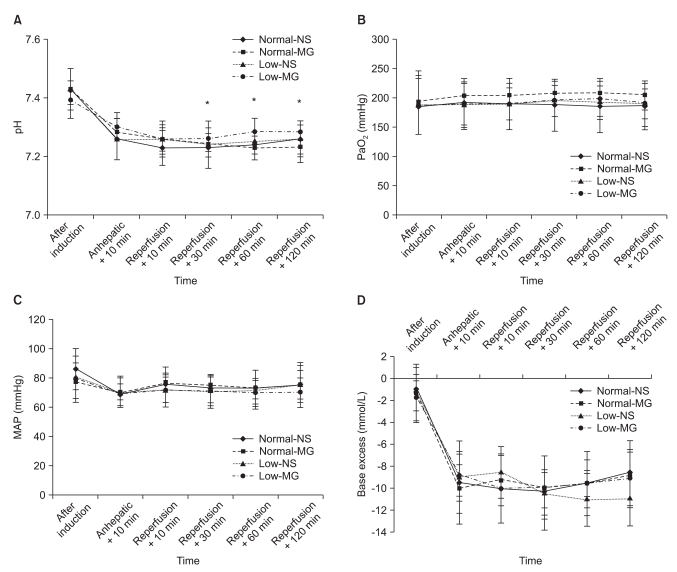
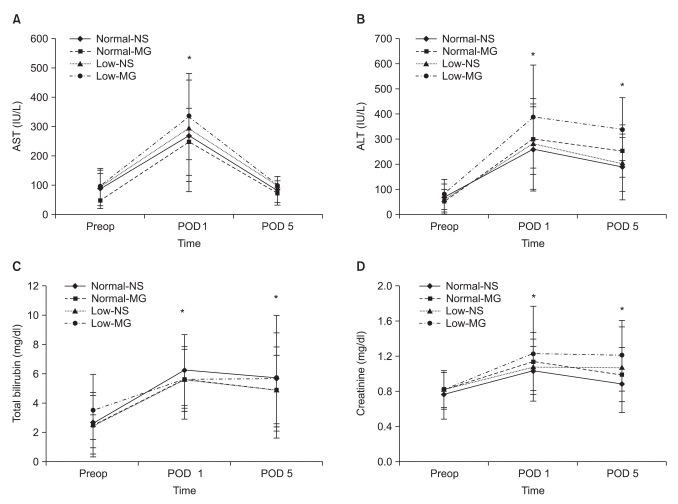
Methods: Fifty-nine living donor liver transplant recipients were randomly assigned to an MG group (n = 31) or an NS group (n = 28). Each group was also divided in two groups based on the preoperative magnesium levels (normal: ≥ 0.70 mmol/L, low: < 0.70 mmol/L). The MG groups received 25 mg/kg of MgSO(4) mixed in 100 ml normal saline intravenously before reperfusion and the NS groups received an equal volume of normal saline. The levels of lactate, pH, arterial oxygen tension, and base excess were measured to assess reperfusion injury at five specific times, which were 10 min after the beginning of anhepatic phase, and 10, 30, 60 and 120 min after reperfusion. To evaluate postoperative organ function, the serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin and creatinine levels were measured at preoperative day 1, postoperative day 1 and 5.
Results: The blood lactate levels were significantly lower at 10, 30, 60 and 120 min after reperfusion in the MG groups compared to the NS groups. In addition, significantly higher blood lactate levels were observed in the NS group with preoperative hypomagnesemia than in MG groups.
Conclusions: Magnesium administration before reperfusion of liver transplantation significantly reduces blood lactate levels. These findings suggest that magnesium treatment may have protective effects on IR injury during living donor liver transplantation.
Keywords: Ischemia reperfusion injury; Lactate; Living donor liver transplantation; Magnesium.
Figures

References
-
- Busuttil RW, Tanaka K. The utility of marginal donors in liver transplantation. Liver Transpl. 2003;9:651–663. - PubMed
-
- Lee SG, Park KM, Hwang S, Lee YJ, Kim KH, Ahn CS, et al. Adult-to-adult living donor liver transplantation at the Asan Medical Center, Korea. Asian J Surg. 2002;25:277–284. - PubMed
-
- Teoh NC, Farrell GC. Hepatic ischemia reperfusion injury: pathogenic mechanisms and basis for hepatoprotection. J Gastroenterol Hepatol. 2003;18:891–902. - PubMed
-
- Fondevila C, Busuttil RW, Kupiec-Weglinski JW. Hepatic ischemia/reperfusion injury--a fresh look. Exp Mol Pathol. 2003;74:86–93. - PubMed
-
- Sakon M, Ariyoshi H, Umeshita K, Monden M. Ischemia-reperfusion injury of the liver with special reference to calcium-dependent mechanisms. Surg Today. 2002;32:1–12. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
