

Changes in Adenosine Deaminase Activity in Patients with Type 2 Diabetes Mellitus and Effect of DPP-4 Inhibitor Treatment on ADA Activity
- PMID: 21738897
- PMCID: PMC3122899
- DOI: 10.4093/dmj.2011.35.2.149
Changes in Adenosine Deaminase Activity in Patients with Type 2 Diabetes Mellitus and Effect of DPP-4 Inhibitor Treatment on ADA Activity
Abstract
Background: Dipeptidyl peptidase 4 (DPP-4, also known as CD26) binds with adenosine deaminase (ADA) to activate T lymphocytes. Here, we investigated whether ADA activity is specifically affected by treatment with DPP-4 inhibitor (DPP4I) compared with other anti-diabetic agents.
Methods: Fasting ADA activity, in addition to various metabolic and biochemical parameters, were measured in 262 type 2 diabetes mellitus (T2DM) patients taking various anti-diabetic agents and in 46 non-diabetic control subjects.
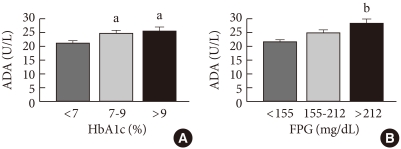
Results: ADA activity was increased in T2DM patients compared with that in non-diabetic control subjects (mean±standard error, 23.1±0.6 U/L vs. 18.6±0.8 U/L; P<0.05). ADA activity was correlated with fasting plasma glucose (r=0.258, P<0.05), HbA1c (r=0.208, P<0.05), aspartate aminotransferase (r=0.325, P<0.05), and alanine aminotransferase (r=0.248, P<0.05). Compared with the well-controlled T2DM patients (HbA1c<7%), the poorly controlled group (HbA1c>9%) showed significantly increased ADA activity (21.1±0.8 U/L vs. 25.4±1.6 U/L; P<0.05). The effect of DPP4I on ADA activity in T2DM patients did not differ from those of other oral anti-diabetic agents or insulin. T2DM patients on metformin monotherapy showed a lower ADA activity (20.9±1.0 U/L vs. 28.1±2.8 U/L; P<0.05) compared with that of those on sulfonylurea monotherapy.
Conclusion: Our results show that ADA activity is increased in T2DM patients compared to that in non-diabetic patients, is positively correlated with blood glucose level, and that DPP4I has no additional specific effect on ADA activity, except for a glycemic control- or HbA1c-dependent effect.
Keywords: Adenosine deaminase; Diabetes mellitus, type 2; Dipeptidyl peptidase.
Figures




Similar articles
-
Adenosine deaminase activity in type 2 diabetes mellitus: does it have any role?BMC Endocr Disord. 2018 Aug 20;18(1):58. doi: 10.1186/s12902-018-0284-9. BMC Endocr Disord. 2018. PMID: 30126383 Free PMC article.
-
Expression of CD26 and its association with dipeptidyl peptidase IV activity in lymphocytes of type 2 diabetes patients.Cell Biochem Biophys. 2011 Nov;61(2):297-302. doi: 10.1007/s12013-011-9212-6. Cell Biochem Biophys. 2011. PMID: 21614532
-
A Prospective Cross-Sectional Study on the Correlation of Adenosine Deaminase and HbA1c With Microvascular Complications in Type 2 Diabetes Mellitus at a Tertiary Care Hospital in Central India.Cureus. 2024 Oct 2;16(10):e70732. doi: 10.7759/cureus.70732. eCollection 2024 Oct. Cureus. 2024. PMID: 39493017 Free PMC article.
-
Clinical pharmacokinetics and pharmacodynamics of vildagliptin.Clin Pharmacokinet. 2012 Mar 1;51(3):147-62. doi: 10.2165/11598080-000000000-00000. Clin Pharmacokinet. 2012. PMID: 22339447 Review.
-
SODIUM GLUCOSE COTRANSPORTER 2 AND DIPEPTIDYL PEPTIDASE-4 INHIBITION: PROMISE OF A DYNAMIC DUO.Endocr Pract. 2017 Jul;23(7):831-840. doi: 10.4158/EP161725.RA. Epub 2017 Mar 23. Endocr Pract. 2017. PMID: 28332871 Review.
Cited by
-
The Adenosinergic System in Diabetic Retinopathy.J Diabetes Res. 2016;2016:4270301. doi: 10.1155/2016/4270301. Epub 2016 Feb 29. J Diabetes Res. 2016. PMID: 27034960 Free PMC article. Review.
-
Gadd45α: a novel diabetes-associated gene potentially linking diabetic cardiomyopathy and baroreflex dysfunction.PLoS One. 2012;7(12):e49077. doi: 10.1371/journal.pone.0049077. Epub 2012 Dec 5. PLoS One. 2012. PMID: 23227140 Free PMC article.
-
Adenosine deaminase, not immune to a mechanistic rethink in central nervous system disorders?Histol Histopathol. 2022 Mar;37(3):189-212. doi: 10.14670/HH-18-404. Epub 2021 Dec 9. Histol Histopathol. 2022. PMID: 34881804 Review.
-
The CD39-adenosinergic axis in the pathogenesis of immune and nonimmune diabetes.J Biomed Biotechnol. 2012;2012:320495. doi: 10.1155/2012/320495. Epub 2012 Oct 14. J Biomed Biotechnol. 2012. PMID: 23118504 Free PMC article. Review.
-
Serum adenosine deaminase activity and coronary artery disease: a retrospective case-control study based on 9929 participants.Ther Adv Chronic Dis. 2019 Dec 6;10:2040622319891539. doi: 10.1177/2040622319891539. eCollection 2019. Ther Adv Chronic Dis. 2019. PMID: 31839921 Free PMC article.
References
-
- Drucker DJ. Enhancing incretin action for the treatment of type 2 diabetes. Diabetes Care. 2003;26:2929–2940. - PubMed
-
- Ahren B. Gut peptides and type 2 diabetes mellitus treatment. Curr Diab Rep. 2003;3:365–372. - PubMed
-
- Zander M, Madsbad S, Madsen JL, Holst JJ. Effect of 6-week course of glucagon-like peptide 1 on glycaemic control, insulin sensitivity, and beta-cell function in type 2 diabetes: a parallel-group study. Lancet. 2002;359:824–830. - PubMed
-
- Drucker DJ. Biological actions and therapeutic potential of the glucagon-like peptides. Gastroenterology. 2002;122:531–544. - PubMed
-
- Nauck MA, Niedereichholz U, Ettler R, Holst JJ, Orskov C, Ritzel R, Schmiegel WH. Glucagon-like peptide 1 inhibition of gastric emptying outweighs its insulinotropic effects in healthy humans. Am J Physiol. 1997;273(5 Pt 1):E981–E988. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
