

Effect of tidal volume, intrathoracic pressure, and cardiac contractility on variations in pulse pressure, stroke volume, and intrathoracic blood volume
- PMID: 21739340
- PMCID: PMC3818902
- DOI: 10.1007/s00134-011-2304-3
Effect of tidal volume, intrathoracic pressure, and cardiac contractility on variations in pulse pressure, stroke volume, and intrathoracic blood volume
Abstract
Purpose: We evaluated the impact of increasing tidal volume (V (t)), decreased chest wall compliance, and left ventricular (LV) contractility during intermittent positive-pressure ventilation (IPPV) on the relation between pulse pressure (PP) and LV stroke volume (SV(LV)) variation (PPV and SVV, respectively), and intrathoracic blood volume (ITBV) changes.
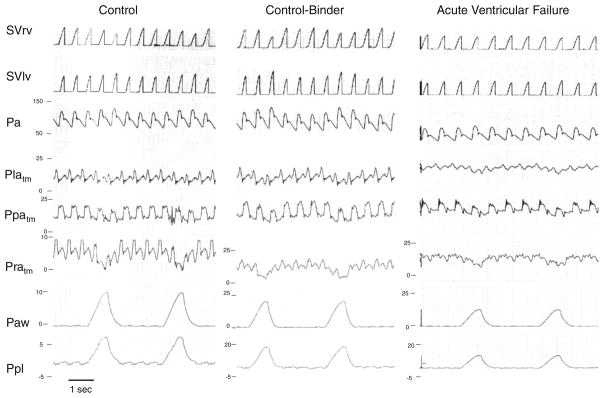
Methods: Sixteen pentobarbital-anesthetized thoracotomized mongrel dogs were studied both before and after propranolol-induced acute ventricular failure (AVF) (n = 4), with and without chest and abdominal pneumatic binders to decrease chest wall compliance (n = 6), and during V (t) of 5, 10, 15, and 25 ml/kg (n = 6). SV(LV) and right ventricular stroke volume (SV(RV)) were derived from electromagnetic flow probes around aortic and pulmonary artery roots. Arterial pressure was measured in the aorta using a fluid-filled catheter. Arterial PPV and SVV were calculated over three breaths as (max - min)/[(max + min)/2]. ITBV changes during ventilation were inferred from the beat-to-beat volume differences between SV(RV) and SV(LV).
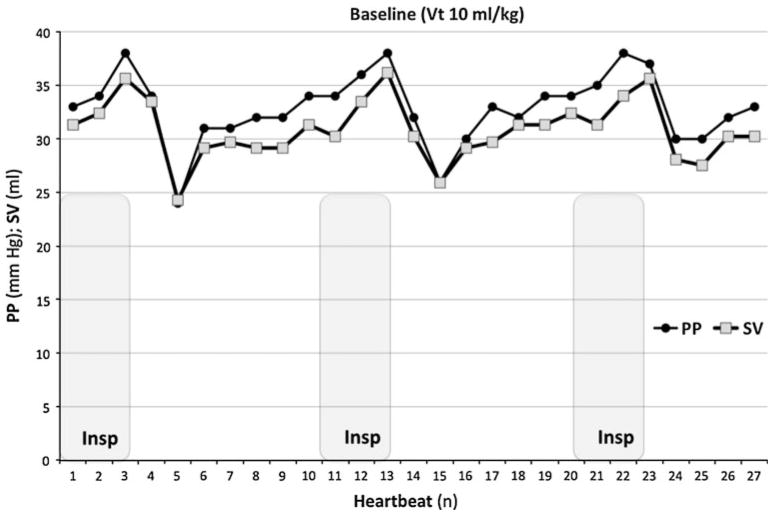
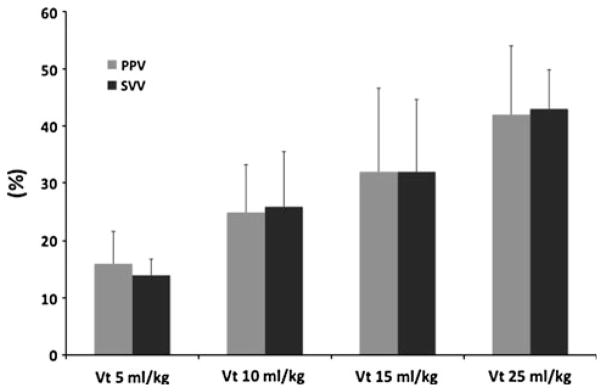
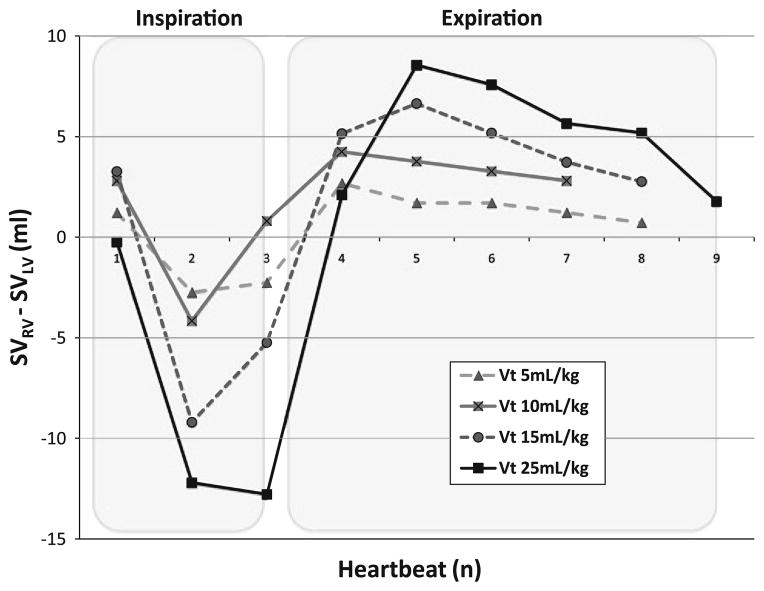
Results: Arterial PP and SV(LV) were tightly correlated during IPPV under all conditions (r (2) = 0.85). Both PPV and SVV increased progressively as V (t) increased and with thoraco-abdominal binding, and tended to decrease during AVF. SV(RV) phasically decreased during inspiration, whereas SV(LV) phasically decreased 2-3 beats later, such that ITBV decreased during inspiration and returned to apneic values during expiration. ITBV decrements increased with increasing V (t) or with thoraco-abdominal binding, and decreased during AVF owing to variations in SV(RV), such that both PPV and SVV tightly correlated with inspiration-associated changes in SV(RV) and ITBV.
Conclusion: Arterial PP and SV(LV) are tightly correlated during IPPV and their relation is not altered by selective changes in LV contractility, intrathoracic pressure, or V (t). However, contractility, intrathoracic pressure, and V (t) directly alter the magnitude of PPV and SVV primarily by altering the inspiration-associated decreases in SV(RV) and ITBV.
Conflict of interest statement
Figures
References
-
- Pinsky MR, Matuschak GM, Klain M. Determinants of cardiac augmentation by increases in intrathoracic pressure. J Appl Physiol. 1985;58:1189–1198. - PubMed
-
- Michard F, Teboul JL. Predicting fluid responsiveness in ICU patients: a critical analysis of the evidence. Chest. 2002;121:2000–2008. - PubMed
-
- Pinsky MR. Using ventilation-induced aortic pressure and flow variation to diagnose preload responsiveness. Intensive Care Med. 2004;30:1008–1010. - PubMed
-
- Michard F, Boussat S, Chemla D, Anguel N, Mercat A, Lecarpentier Y, Richard C, Pinsky MR, Teboul JL. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162:134–138. - PubMed
-
- Reuter DA, Felbinger TW, Schmidt C, Kilger E, Goedje O, Lamm P, Goetz AE. Stroke volume variation for assessment of cardiac responsiveness to volume loading in mechanically ventilated patients after cardiac surgery. Intensive Care Med. 2002;28:392–398. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
