

Ranolazine reduces Ca2+ overload and oxidative stress and improves mitochondrial integrity to protect against ischemia reperfusion injury in isolated hearts
- PMID: 21741479
- PMCID: PMC3233383
- DOI: 10.1016/j.phrs.2011.06.018
Ranolazine reduces Ca2+ overload and oxidative stress and improves mitochondrial integrity to protect against ischemia reperfusion injury in isolated hearts
Abstract
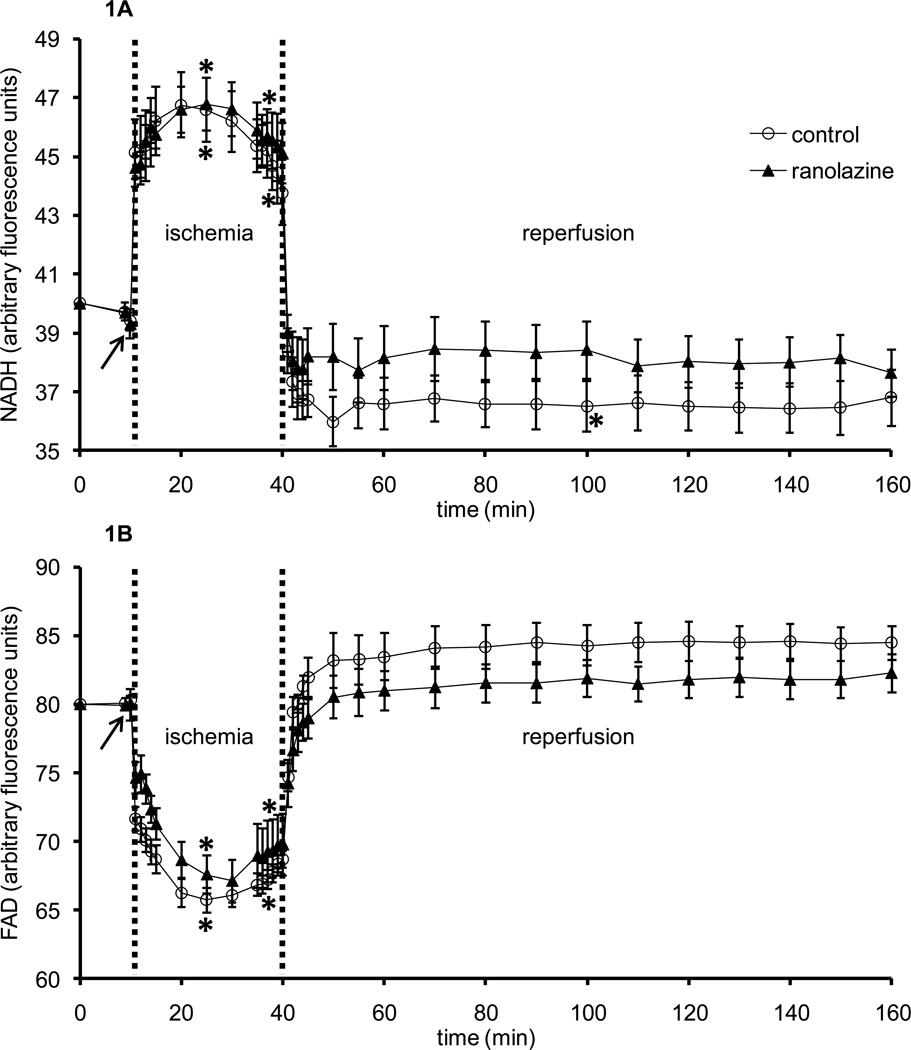
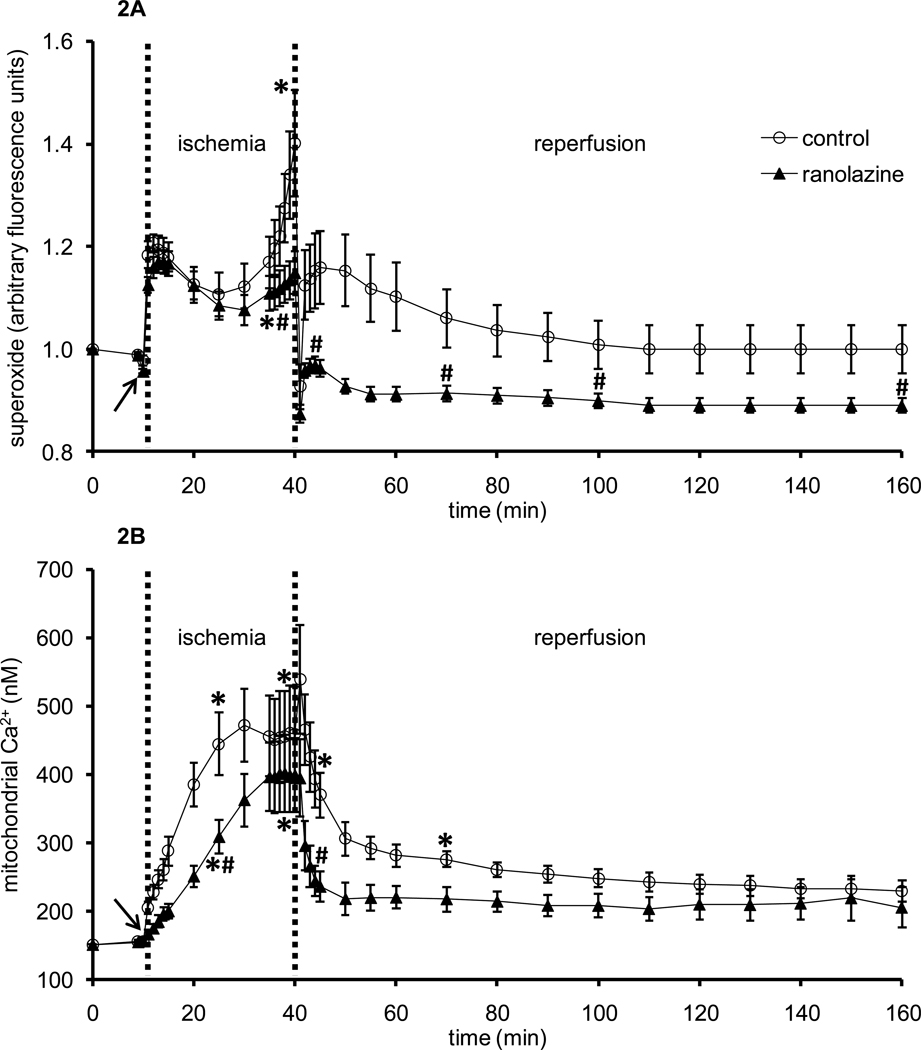
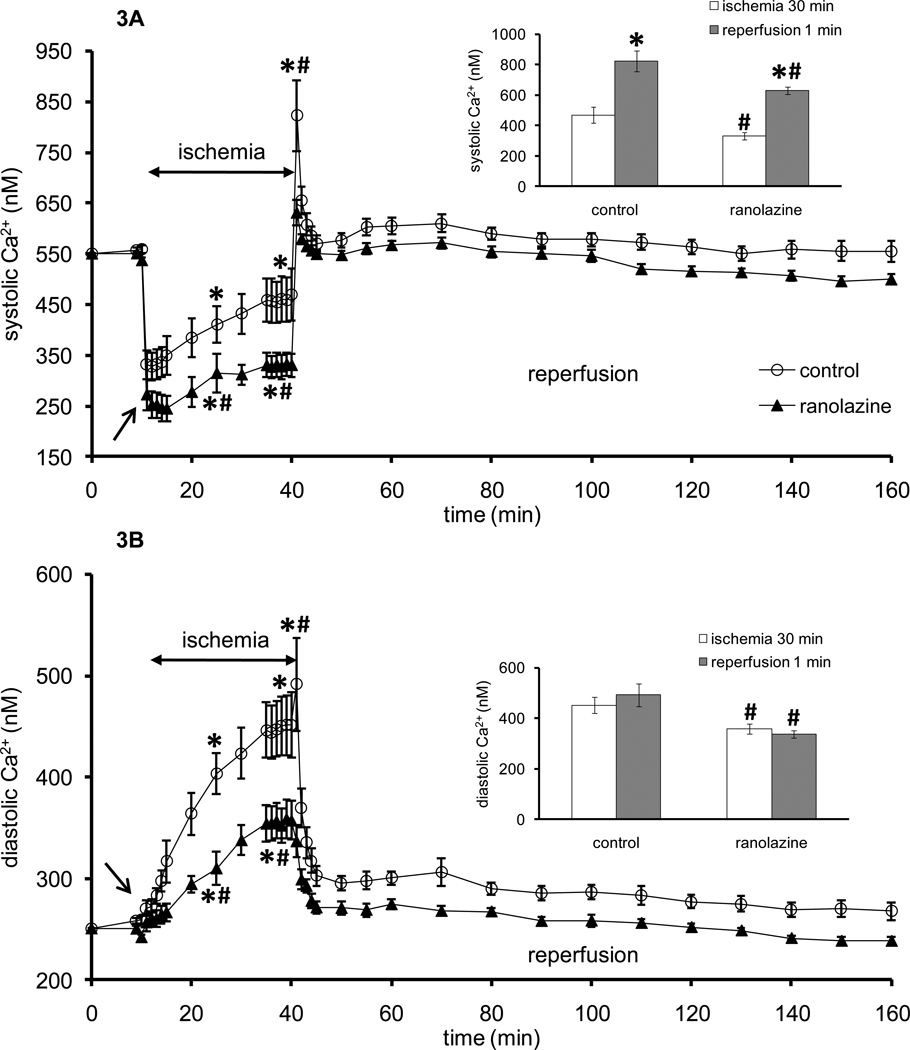
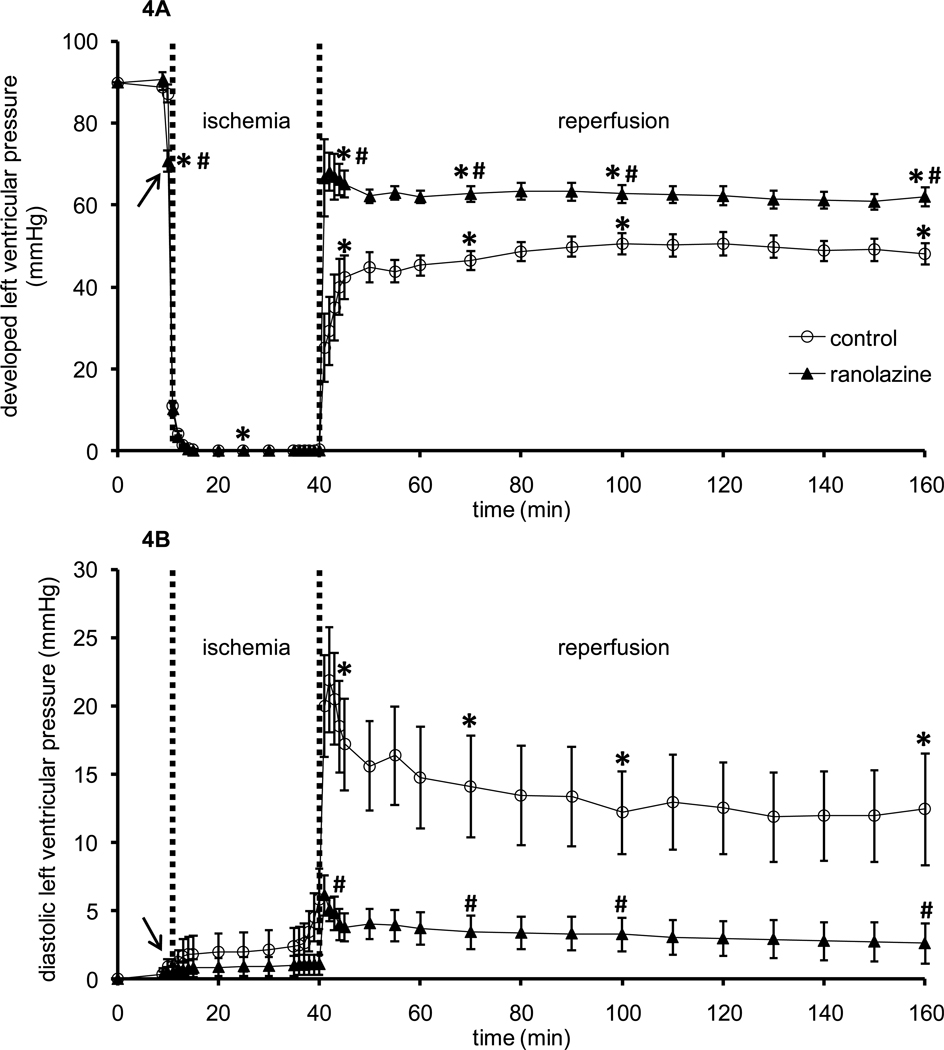
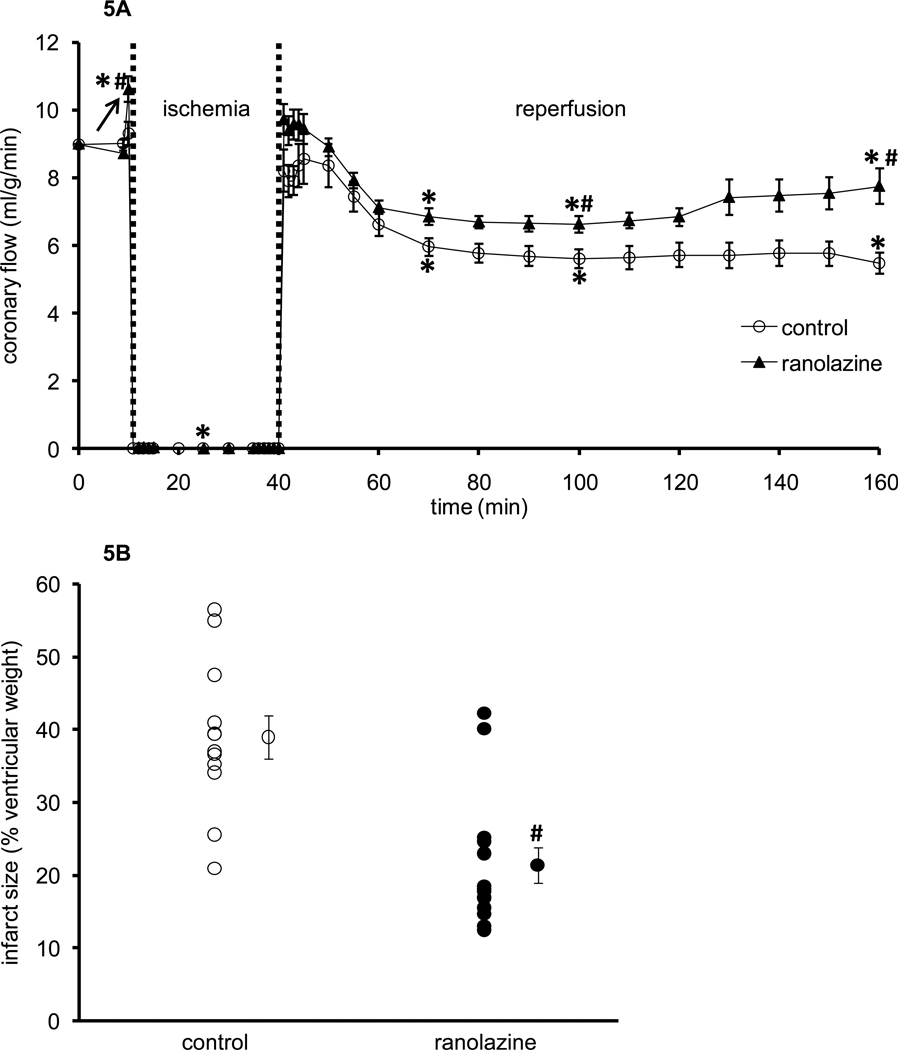
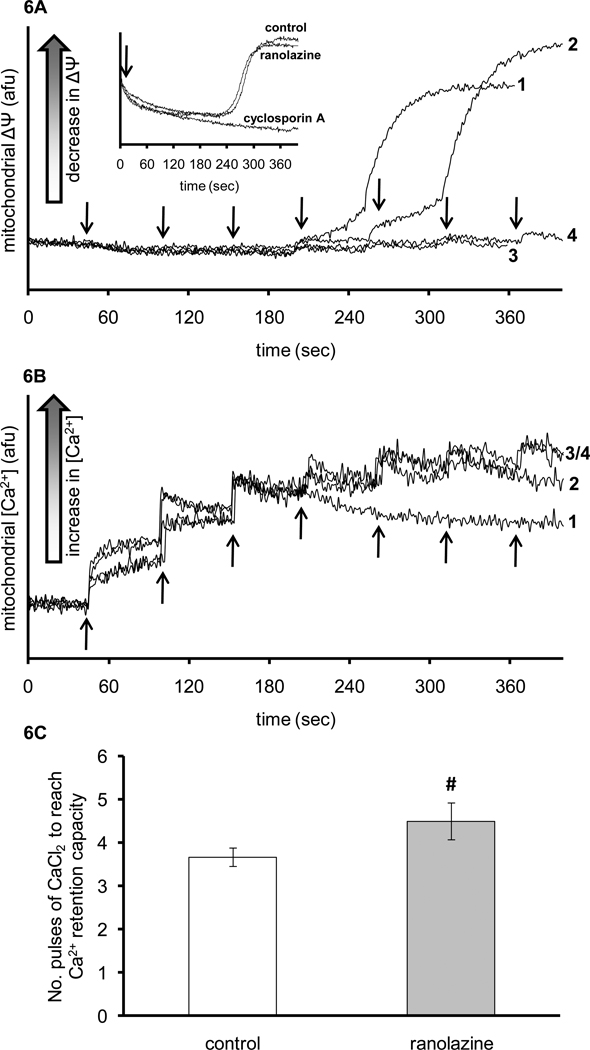
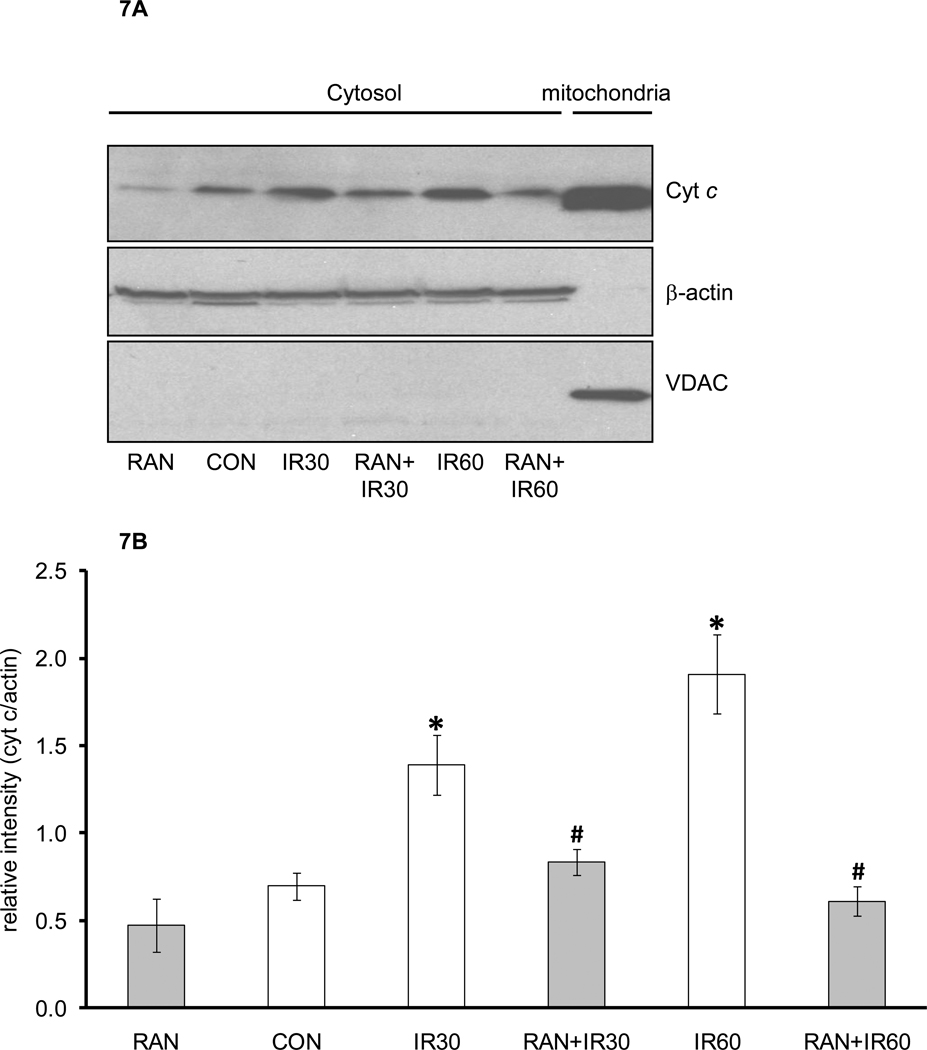
Ranolazine is a clinically approved drug for treating cardiac ventricular dysrhythmias and angina. Its mechanism(s) of protection is not clearly understood but evidence points to blocking the late Na+ current that arises during ischemia, blocking mitochondrial complex I activity, or modulating mitochondrial metabolism. Here we tested the effect of ranolazine treatment before ischemia at the mitochondrial level in intact isolated hearts and in mitochondria isolated from hearts at different times of reperfusion. Left ventricular (LV) pressure (LVP), coronary flow (CF), and O2 metabolism were measured in guinea pig isolated hearts perfused with Krebs-Ringer's solution; mitochondrial (m) superoxide (O2·-), Ca2+, NADH/FAD (redox state), and cytosolic (c) Ca2+ were assessed on-line in the LV free wall by fluorescence spectrophotometry. Ranolazine (5 μM), infused for 1 min just before 30 min of global ischemia, itself did not change O2·-, cCa2+, mCa2+ or redox state. During late ischemia and reperfusion (IR) O2·- emission and m[Ca2+] increased less in the ranolazine group vs. the control group. Ranolazine decreased c[Ca2+] only during ischemia while NADH and FAD were not different during IR in the ranolazine vs. control groups. Throughout reperfusion LVP and CF were higher, and ventricular fibrillation was less frequent. Infarct size was smaller in the ranolazine group than in the control group. Mitochondria isolated from ranolazine-treated hearts had mild resistance to permeability transition pore (mPTP) opening and less cytochrome c release than control hearts. Ranolazine may provide functional protection of the heart during IR injury by reducing cCa2+ and mCa2+ loading secondary to its effect to block the late Na+ current. Subsequently it indirectly reduces O2·- emission, preserves bioenergetics, delays mPTP opening, and restricts loss of cytochrome c, thereby reducing necrosis and apoptosis.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest: None.
Figures
References
-
- Yellon DM, Hausenloy DJ. Myocardial reperfusion injury. N Engl J Med. 2007;357:1121–1135. - PubMed
-
- Jennings RB, Sommers HM, Smyth GA, Flack HA, Linn H. Myocardial necrosis induced by temporary occlusion of a coronary artery in the dog. Arch Pathol. 1960;70:68–78. - PubMed
-
- Mewton N, Ivanes F, Cour M, Ovize M. Postconditioning: from experimental proof to clinical concept. Dis Model Mech. 2010;3:39–44. - PubMed
-
- Chen Q, Camara AK, Stowe DF, Hoppel CL, Lesnefsky EJ. Modulation of electron transport protects cardiac mitochondria and decreases myocardial injury during ischemia and reperfusion. Am J Physiol Cell Physiol. 2007;292:C137–C147. - PubMed
-
- Becker LB, vanden Hoek TL, Shao ZH, Li CQ, Schumacker PT. Generation of superoxide in cardiomyocytes during ischemia before reperfusion. Am J Physiol. 1999;277:H2240–H2246. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
