

Holoprosencephaly: a guide to diagnosis and clinical management
- PMID: 21743112
- PMCID: PMC4131946
- DOI: 10.1007/s13312-011-0078-x
Holoprosencephaly: a guide to diagnosis and clinical management
Abstract
Context: Holoprosencephaly affects 1 in 8,000 live births and is the most common structural anomaly of the developing forebrain, resulting in facial dysmorphism, neurologic impairment, and additional clinical sequelae. Given the increasing relative contribution of genetic diseases to perinatal morbidity and mortality in India, proper recognition and management of holoprosencephaly can improve care for a significant number of affected Indian children.
Evidence acquisition: We used the PubMed database (search terms: "holoprosencephaly," "HPE," "holoprosencephaly India") and cross-referenced articles regarding holoprosencephaly, using our research group's extensive experience as a guide for identifying seminal papers in the field.
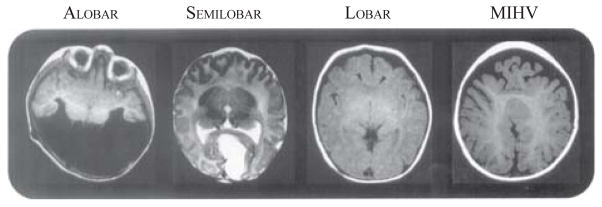
Results: Holoprosencephaly is classified into four types based on the nature of the brain malformations as seen on neuroimaging and/or pathologic examination, with typically recognizable craniofacial phenotypes. Despite the identification of several genetic loci and other etiologic agents involved in pathogenesis, additional causes are elusive. Moreover, satisfactory explanations for phenomena such as incomplete penetrance and variable expressivity are lacking.
Conclusions: For each patient, pediatricians should follow a diagnostic protocol including dysmorphology examination, complete family history and ascertainment of risk factors, and neuroimaging. Many medical issues, including hypothalamic dysfunction, endocrinologic dysfunction, motor impairment, respiratory issues, seizures, and hydrocephalus should be prioritized in management. Pediatricians should work with genetic specialists to identify syndromic forms and to perform cytogenetic investigation, molecular screening, and genetic counseling in order to fully characterize prognosis and recurrence risk.
Conflict of interest statement
Figures


References
-
- O’Rahilly R, Müller F. Interpretation of some median anomalies as illustrated by cyclopia and symmelia. Teratology. 1989;40:409–21. - PubMed
-
- Matsunaga E, Shiota K. Holoprosencephaly in human embryos: epidemiologic studies of 150 cases. Teratology. 1977;16:261–72. - PubMed
-
- Leoncini E, Baranello G, Orioli IM, Annerén G, Bakker M, Bianchi F, et al. Frequency of holoprosencephaly in the International Clearinghouse Birth Defects Surveillance systems: searching for population variations. Birth Defects Res A. 2008;82:585–91. - PubMed
-
- Orioli IM, Castilla EE. Epidemiology of holoprosencephaly: prevalence and risk factors. Am J Med Genet C Semin Med Genet. 2010;154C:13–21. - PubMed
-
- Thakur S, Singh R, Pradhan M, Phadke SR. Spectrum of holoprosencephaly. Indian J Pediatr. 2004;71:593–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources