

Somatotroph pituitary adenoma with acromegaly and autosomal dominant polycystic kidney disease: SSTR5 polymorphism and PKD1 mutation
- PMID: 21744088
- PMCID: PMC3905832
- DOI: 10.1007/s11102-011-0325-0
Somatotroph pituitary adenoma with acromegaly and autosomal dominant polycystic kidney disease: SSTR5 polymorphism and PKD1 mutation
Abstract
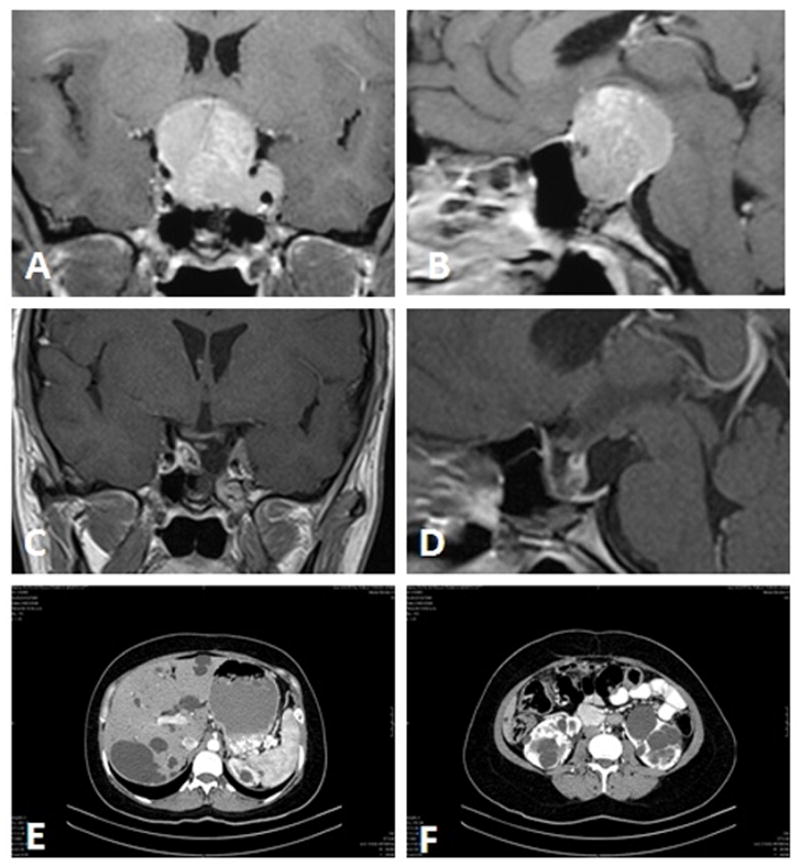
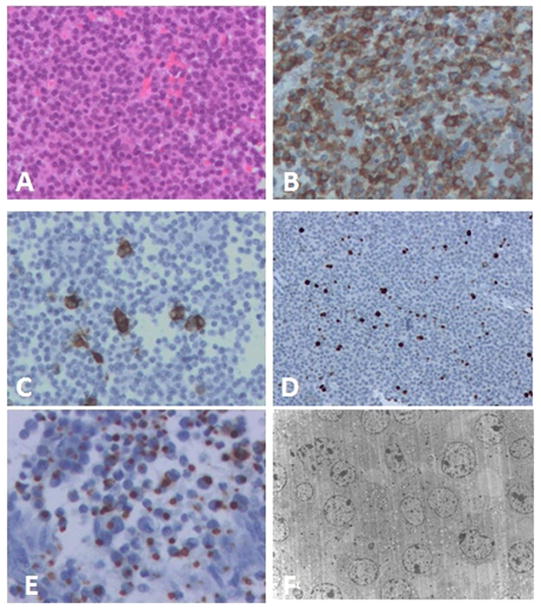
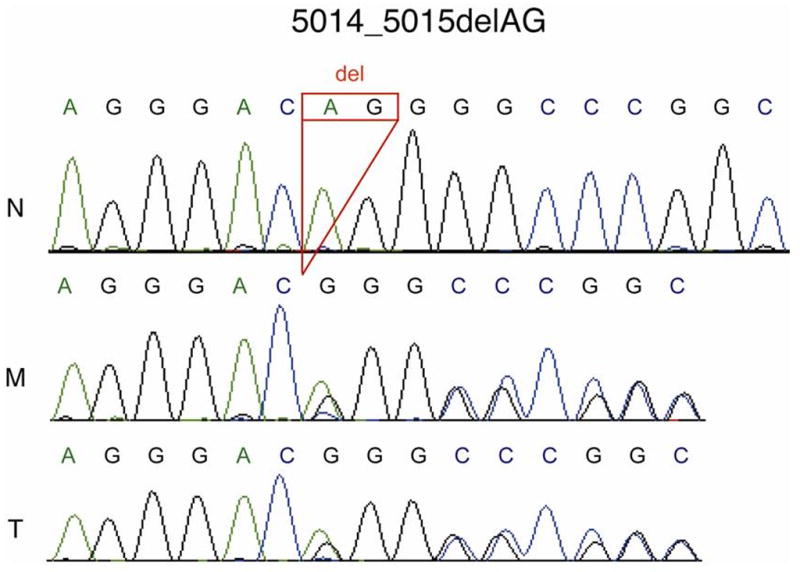
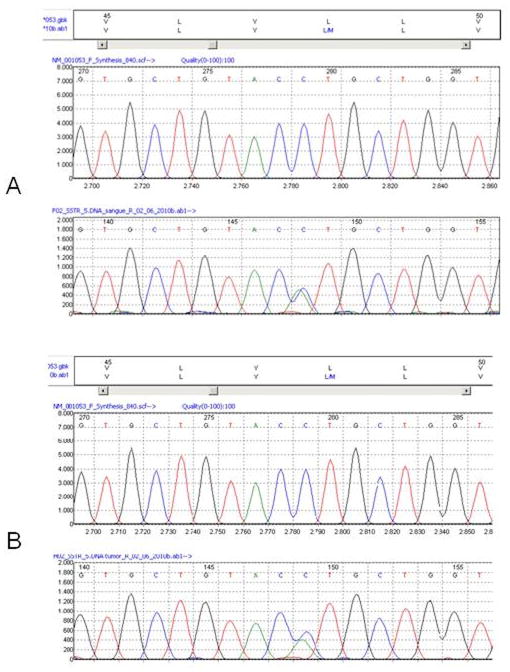
A 39-year-old woman with autosomal dominant polycystic kidney disease (ADPKD) presented with acromegaly and a pituitary macroadenoma. There was a family history of this renal disorder. She had undergone surgery for pituitary adenoma 6 years prior. Physical examination disclosed bitemporal hemianopsia and elevation of both basal growth hormone (GH) 106 ng/mL (normal 0-5) and insulin-like growth factor (IGF-1) 811 ng/mL (normal 48-255) blood levels. A magnetic resonance imaging scan disclosed a 3.0 cm sellar and suprasellar mass with both optic chiasm compression and left cavernous sinus invasion. Pathologic, cytogenetic, molecular and in silico analysis was undertaken. Histologic, immunohistochemical and ultrastructural studies of the lesion disclosed a sparsely granulated somatotroph adenoma. Standard chromosome analysis on the blood sample showed no abnormality. Sequence analysis of the coding regions of PKD1 and PKD2 employing DNA from both peripheral leukocytes and the tumor revealed the most common PKD1 mutation, 5014_5015delAG. Analysis of the entire SSTR5 gene disclosed the variant c.142C>A (p.L48M, rs4988483) in the heterozygous state in both blood and tumor, while no pathogenic mutations were noted in the MEN1, AIP, p27Kip1 and SSTR2 genes. To our knowledge, this is the fourth reported case of a GH-producing pituitary adenoma associated with ADPKD, but the first subjected to extensive morphological, ultrastructural, cytogenetic and molecular studies. The physical proximity of the PKD1 and SSTR5 genes on chromosome 16 suggests a causal relationship between ADPKD and somatotroph adenoma.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
