

Cardiac disease in patients with mucopolysaccharidosis: presentation, diagnosis and management
- PMID: 21744090
- PMCID: PMC3228957
- DOI: 10.1007/s10545-011-9359-8
Cardiac disease in patients with mucopolysaccharidosis: presentation, diagnosis and management
Abstract
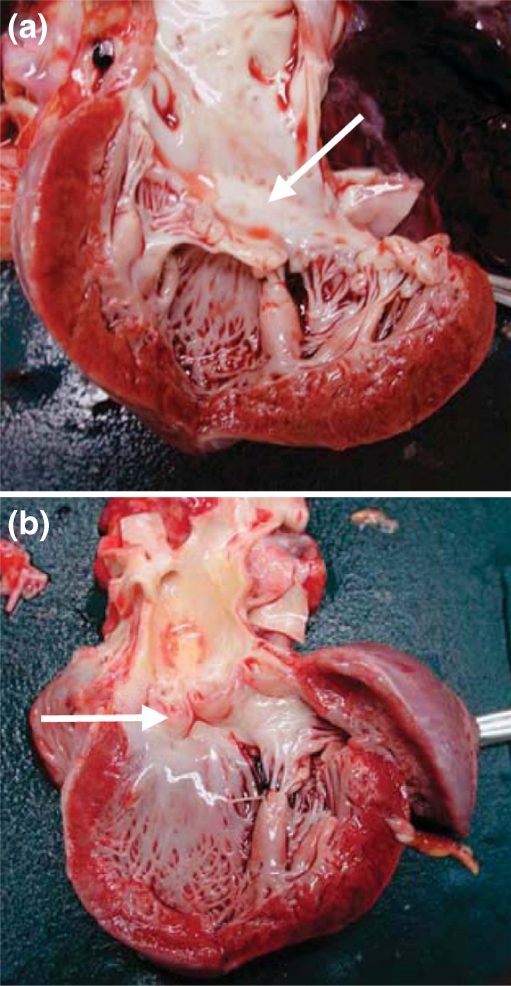
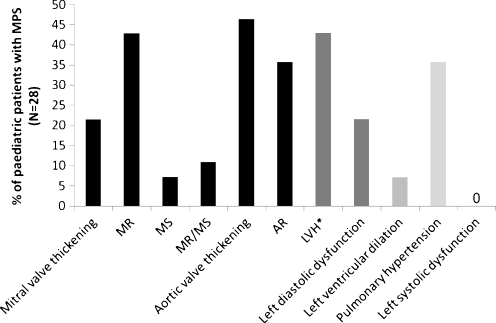
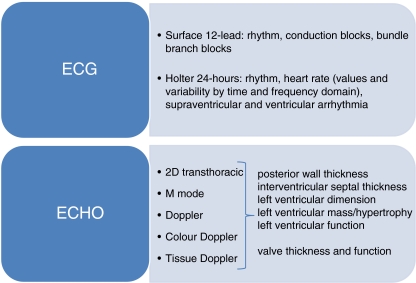
The mucopolysaccharidoses (MPSs) are inherited lysosomal storage disorders caused by the absence of functional enzymes that contribute to the degradation of glycosaminoglycans (GAGs). The progressive systemic deposition of GAGs results in multi-organ system dysfunction that varies with the particular GAG deposited and the specific enzyme mutation(s) present. Cardiac involvement has been reported in all MPS syndromes and is a common and early feature, particularly for those with MPS I, II, and VI. Cardiac valve thickening, dysfunction (more severe for left-sided than for right-sided valves), and hypertrophy are commonly present; conduction abnormalities, coronary artery and other vascular involvement may also occur. Cardiac disease emerges silently and contributes significantly to early mortality.The clinical examination of individuals with MPS is often difficult due to physical and, sometimes, intellectual patient limitations. The absence of precordial murmurs does not exclude the presence of cardiac disease. Echocardiography and electrocardiography are key diagnostic techniques for evaluation of valves, ventricular dimensions and function, which are recommended on a regular basis. The optimal technique for evaluation of coronary artery involvement remains unsettled.Standard medical and surgical techniques can be modified for MPS patients, and systemic therapies such as hematopoietic stem cell transplantation and enzyme replacement therapy (ERT) may alter overall disease progression with regression of ventricular hypertrophy and maintenance of ventricular function. Cardiac valve disease is usually unresponsive or, at best, stabilized, although ERT within the first few months of life may prevent valve involvement, a fact that emphasizes the importance of early diagnosis and treatment in MPS.
Figures



References
-
- Barry MO, Beardslee MA, Braverman AC. Morquio’s syndrome: severe aortic regurgitation and late pulmonary autograft failure. J Heart Valve Dis. 2006;15:839–842. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
