

Rates of, and risk factors for, severe infections in patients with systemic autoimmune diseases receiving biological agents off-label
- PMID: 21745378
- PMCID: PMC3239350
- DOI: 10.1186/ar3397
Rates of, and risk factors for, severe infections in patients with systemic autoimmune diseases receiving biological agents off-label
Abstract
Introduction: The purpose of this observational study was to analyze the rates, characteristics and associated risk factors of severe infections in patients with systemic autoimmune diseases (SAD) who were treated off-label with biological agents in daily practice.
Methods: The BIOGEAS registry is an ongoing Spanish prospective cohort study investigating the long-term safety and efficacy of the off-label use of biological agents in adult patients with severe, refractory SAD. Severe infections were defined according to previous studies as those that required intravenous treatment or that led to hospitalization or death. Patients contributed person-years of follow-up for the period in which they were treated with biological agents.
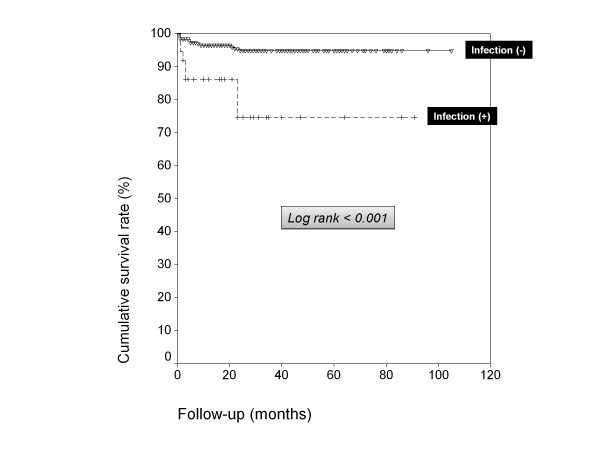
Results: A total of 344 patients with SAD treated with biological agents off-label were included in the Registry until July 2010. The first biological therapies included rituximab in 264 (77%) patients, infliximab in 37 (11%), etanercept in 21 (6%), adalimumab in 19 (5%), and 'other' agents in 3 (1%). Forty-five severe infections occurred in 37 patients after a mean follow-up of 26.76 months. These infections resulted in four deaths. The crude rate of severe infections was 90.9 events/1000 person-years (112.5 for rituximab, 76.9 for infliximab, 66.9 for adalimumab and 30.5 for etanercept respectively). In patients treated with more than two courses of rituximab, the crude rate of severe infection was 226.4 events/1000 person-years. A pathogen was identified in 24 (53%) severe infections. The most common sites of severe infection were the lower respiratory tract (39%), bacteremia/sepsis (20%) and the urinary tract (16%). There were no significant differences relating to gender, SAD, agent, other previous therapies, number of previous immunosuppressive agents received or other therapies administered concomitantly. Cox regression analysis showed that age (P = 0.015) was independently associated with an increased risk of severe infection. Survival curves showed a lower survival rate in patients with severe infections (log-rank and Breslow tests < 0.001).
Conclusions: The rates of severe infections in SAD patients with severe, refractory disease treated depended on the biological agent used, with the highest rates being observed for rituximab and the lowest for etanercept. The rate of infection was especially high in patients receiving three or more courses of rituximab. In patients with severe infections, survival was significantly reduced. Older age was the only significant predictive factor of severe infection.
Figures
References
-
- Meijer JM, Meiners PM, Vissink A, Spijkervet FK, Abdulahad W, Kamminga N, Brouwer E, Kallenberg CG, Bootsma H. Effectiveness of rituximab treatment in primary Sjögren's syndrome: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2010;62:960–968. - PubMed
-
- Dass S, Bowman SJ, Vital EM, Ikeda K, Pease CT, Hamburger J, Richards A, Rauz S, Emery P. Reduction of fatigue in Sjögren syndrome with rituximab: results of a randomised, double-blind, placebo-controlled pilot study. Ann Rheum Dis. 2008;67:1541–1544. - PubMed
-
- Merrill JT, Neuwelt CM, Wallace DJ, Shanahan JC, Latinis KM, Oates JC, Utset TO, Gordon C, Isenberg DA, Hsieh HJ, Zhang D, Brunetta PG. Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: the randomized, double-blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. 2010;62:222–233. doi: 10.1002/art.27233. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
