

Management of pediatric chest pain using a standardized assessment and management plan
- PMID: 21746719
- PMCID: PMC9923781
- DOI: 10.1542/peds.2011-0141
Management of pediatric chest pain using a standardized assessment and management plan
Abstract
Objectives: Chest pain is a common reason for referral to pediatric cardiologists and often leads to an extensive cardiac evaluation. The objective of this study is to describe current management practices in the assessment of pediatric chest pain and to determine whether a standardized care approach could reduce unnecessary testing.
Patients and methods: We reviewed all patients, aged 7 to 21 years, presenting to our outpatient pediatric cardiology division in 2009 for evaluation of chest pain. Demographics, clinical characteristics, patient outcomes, and resource use were analyzed.
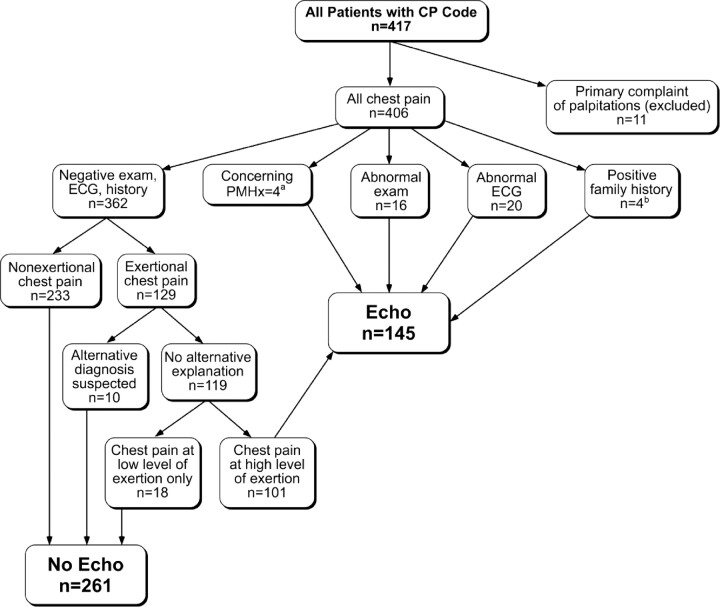
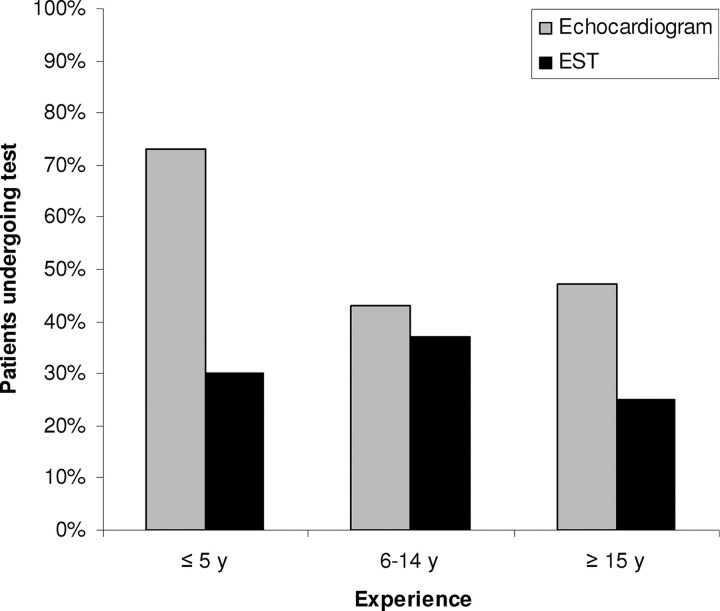
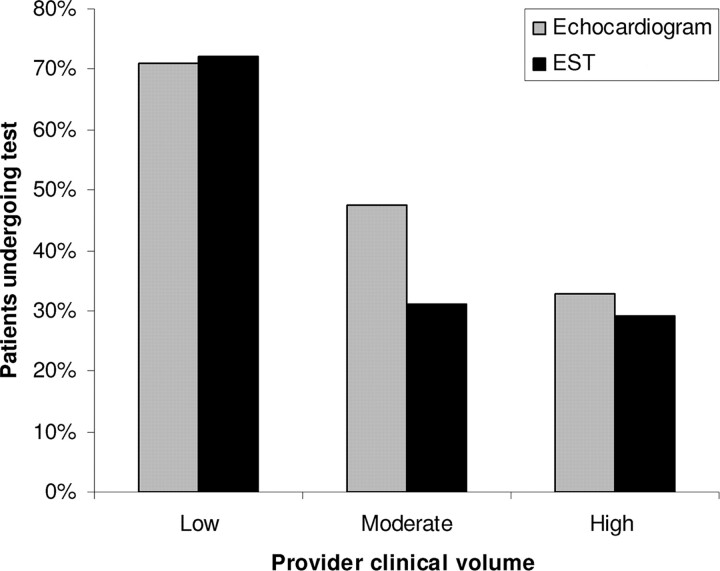
Results: Testing included electrocardiography (ECG) in all 406 patients, echocardiography in 175 (43%), exercise stress testing in 114 (28%), event monitoring in 40 (10%), and Holter monitoring in 30 (7%). A total of 44 (11%) patients had a clinically significant medical or family history, an abnormal cardiac examination, and/or an abnormal ECG. Exertional chest pain was present in 150 (37%) patients. In the entire cohort, a cardiac etiology for chest pain was found in only 5 of 406 (1.2%) patients. Two patients had pericarditits, and 3 had arrhythmias. We developed an algorithm using pertinent history, physical examination, and ECG findings to suggest when additional testing is indicated. Applying the algorithm to this cohort could lead to an ∼20% reduction in echocardiogram and outpatient rhythm monitor use and elimination of exercise stress testing while still capturing all cardiac diagnoses.
Conclusions: Evaluation of pediatric chest pain is often extensive and rarely yields a cardiac etiology. Practice variation and unnecessary resource use remain concerns. Targeted testing can reduce resource use and lead to more cost-effective care.
Conflict of interest statement
Figures
Comment in
-
Majority of children with chest pain do not have an underlying cardiac cause.J Pediatr. 2012 Jan;160(1):176. doi: 10.1016/j.jpeds.2011.11.017. J Pediatr. 2012. PMID: 22152208 No abstract available.
References
-
- Balfour IC , Rao PS . Chest pain in children. Indian J Pediatr. 1998;65(1):21–26 - PubMed
-
- Evangelista JA , Parsons M , Renneburg AK . Chest pain in children: diagnosis through history and physical examination. J Pediatr Health Care. 2000;14(1):3–8 - PubMed
-
- Tunaoglu FS , Olgunturk R , Akcabay S , Oguz D , Gucuyener K , Demirsoy S . Chest pain in children referred to a cardiology clinic. Pediatr Cardiol. 1995;16(2):69–72 - PubMed
-
- Zavaras-Angelidou KA , Weinhouse E , Nelson DB . Review of 180 episodes of chest pain in 134 children. Pediatr Emerg Care. 1992;8(4):189–193 - PubMed
-
- Cava JR , Sayger PL . Chest pain in children and adolescents. Pediatr Clin North Am. 2004;51(6):1553–1568, viii - PubMed
