

Epidemiology of apnea and bradycardia resolution in premature infants
- PMID: 21746726
- PMCID: PMC3387856
- DOI: 10.1542/peds.2010-1567
Epidemiology of apnea and bradycardia resolution in premature infants
Abstract
Background: There is little epidemiologic evidence to assess the maturation of respiratory control in premature infants.
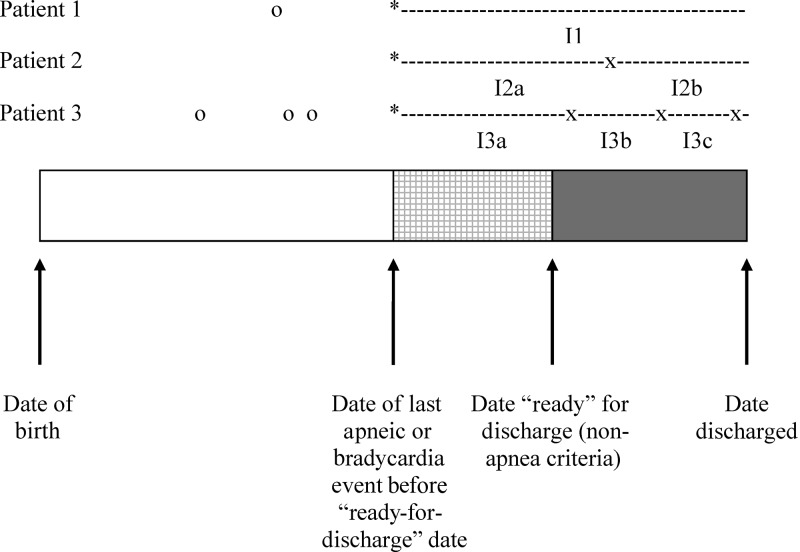
Objective: To measure the success rate or the percentage of infants who have no additional events of various apnea- or bradycardia-free intervals after correcting for gestational age, postmenstrual age of the last apnea or bradycardia event, and the severity of the event.
Methods: This was a retrospective cohort study of infants born at 34 weeks' gestational age or earlier at 1 of 5 Kaiser Permanente Medical Care Program hospitals between 1998 and 2001. The success rates of various apnea- or bradycardia-free intervals were calculated after stratifying according to gestational age, postmenstrual age of the last event, or event severity.
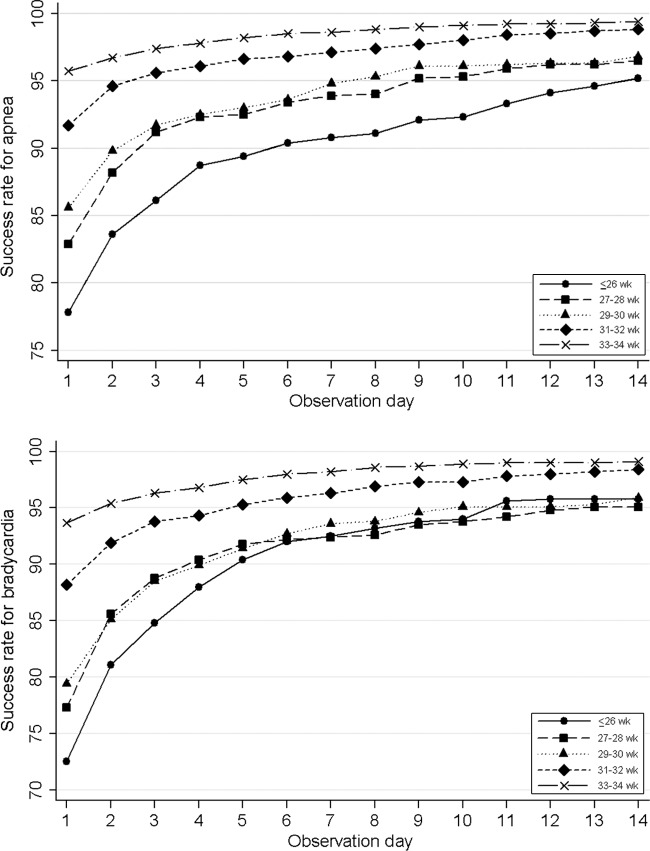
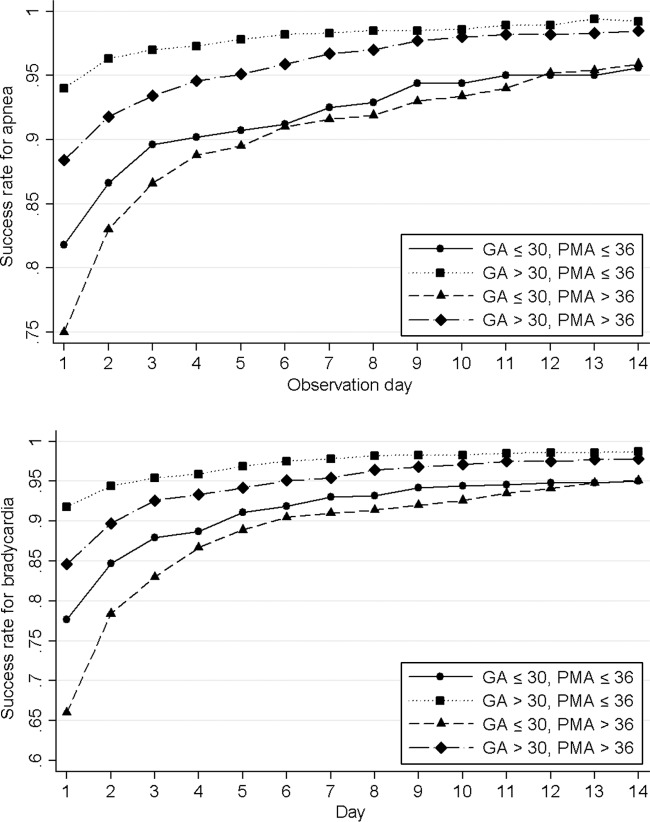
Results: Among the 1403 infants identified in this study, 84.2% did not have an apnea event and 78.5% did not have a bradycardia event after they were otherwise ready for discharge. For the entire cohort, a 95% success rate was statistically reached, with a 7-day apnea- or bradycardia-free interval. Infants with a gestational age of 30 weeks or less had a 5% to 15% lower success rate than infants with a gestational age more than 30 weeks for any given apnea- or bradycardia-free interval. The success rate was reduced by an additional 5% to 10% if the last apnea or bradycardia event occurred at a postmenstrual age of more than 36 weeks. Including only the most severe events slightly improved the success rate of a given interval.
Conclusions: The risk of recurrence for apnea or bradycardia differs depending on the gestational age of the infant and the postmenstrual age of the last apnea or bradycardia event.
Figures
References
-
- American Academy of Pediatrics, Committee on Fetus and Newborn Hospital discharge of the high-risk neonate. Pediatrics. 2008;122(5):1119–1126 - PubMed
-
- Bakewell-Sachs S, Medoff-Cooper B, Escobar GJ, et al. Infant functional status: the timing of physiologic maturation of premature infants. Pediatrics. 2009;123(5). Available at: www.pediatrics.org/cgi/content/full/123/5/e878 - PubMed
-
- Henderson-Smart DJ. The effect of gestational age on the incidence and duration of recurrent apnoea in newborn babies. Aust Paediatr J. 1981;17(4):273–276 - PubMed
-
- Eichenwald EC, Aina A, Stark AR. Apnea frequently persists beyond term gestation in infants delivered at 24 to 28 weeks. Pediatrics. 1997;100(3 pt 1):354–359 - PubMed
-
- Ramanathan R, Corwin MJ, Hunt CE, et al. Cardiorespiratory events recorded on home monitors: comparison of healthy infants with those at increased risk for SIDS. JAMA. 2001;285(17):2199–2207 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
