

Telehealthcare for asthma: a Cochrane review
- PMID: 21746825
- PMCID: PMC3153544
- DOI: 10.1503/cmaj.101146
Telehealthcare for asthma: a Cochrane review
Abstract
Background: Telehealthcare has the potential to provide care for long-term conditions that are increasingly prevalent, such as asthma. We conducted a systematic review of studies of telehealthcare interventions used for the treatment of asthma to determine whether such approaches to care are effective.
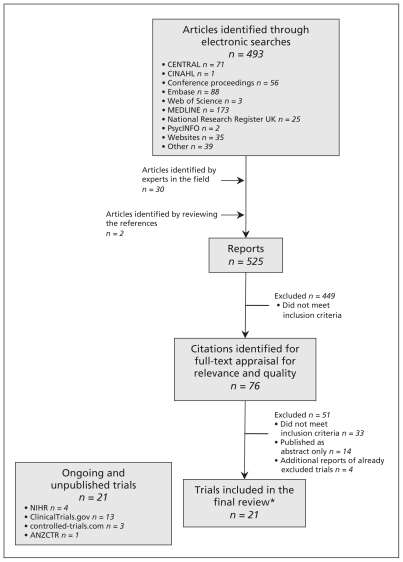
Methods: We searched the Cochrane Airways Group Specialised Register of Trials, which is derived from systematic searches of bibliographic databases including CENTRAL (the Cochrane Central Register of Controlled Trials), MEDLINE, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature) and PsycINFO, as well as other electronic resources. We also searched registers of ongoing and unpublished trials. We were interested in studies that measured the following outcomes: quality of life, number of visits to the emergency department and number of admissions to hospital. Two reviewers identified studies for inclusion in our meta-analysis. We extracted data and used fixedeffect modelling for the meta-analyses.
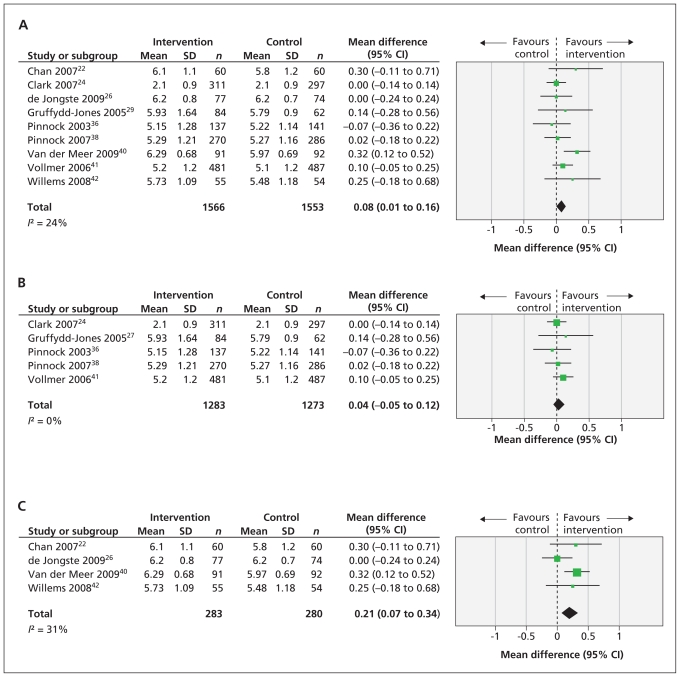
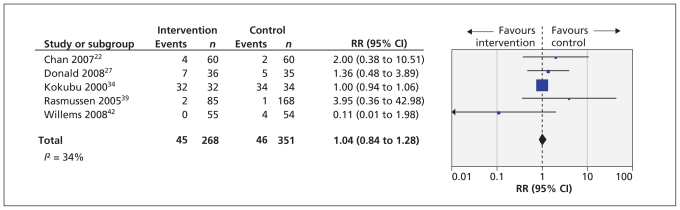
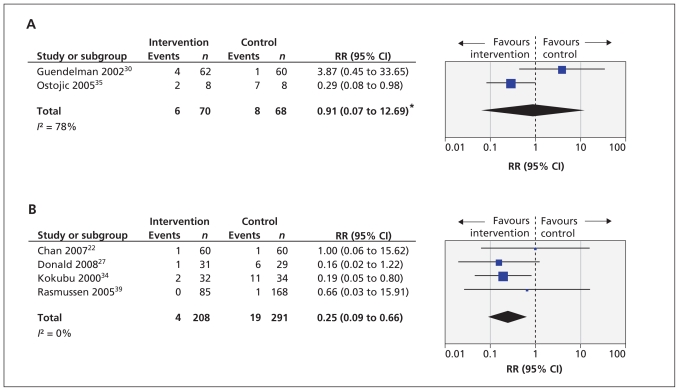
Results: We identified 21 randomized controlled trials for inclusion in our analysis. The methods of telehealthcare intervention these studies investigated were the telephone and video- and Internet-based models of care. Meta-analysis did not show a clinically important improvement in patients' quality of life, and there was no significant change in the number of visits to the emergency department over 12 months. There was a significant reduction in the number of patients admitted to hospital once or more over 12 months (risk ratio 0.25 [95% confidence interval 0.09 to 0.66]).
Interpretation: We found no evidence of a clinically important impact on patients' quality of life, but telehealthcare interventions do appear to have the potential to reduce the risk of admission to hospital, particularly for patients with severe asthma. Further research is required to clarify the cost-effectiveness of models of care based on telehealthcare.
Figures
References
-
- Pearce N, Sunyer J, Cheng S, et al. Comparison of asthma prevalence in the ISAAC and the ECRHS. Eur Respir J 2000; 16:420–6 - PubMed
-
- Asher MI, Montefore S, Bjorkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma allergic rhinoconjunctivitis and eczema in childhood: ISAAC Phases One and Three repeat muli-country cross-sectional surveys. Lancet 2006;368: 733–43 - PubMed
-
- Masoli M, Fabian D, Holt S, et al. Global burden of asthma. GINA [The Global Initiative for Asthma]; 2003 - PubMed
-
- The future of asthma. Lancet 1997;350:1113. - PubMed