

Grating visual acuity results in the early treatment for retinopathy of prematurity study
- PMID: 21746974
- PMCID: PMC4374597
- DOI: 10.1001/archophthalmol.2011.143
Grating visual acuity results in the early treatment for retinopathy of prematurity study
Abstract
Objective: To compare grating (resolution) visual acuity at 6 years of age in eyes that received early treatment (ET) for high-risk prethreshold retinopathy of prematurity (ROP) with that in eyes that underwent conventional management (CM).
Methods: In a randomized clinical trial, infants with bilateral, high-risk prethreshold ROP (n = 317) had one eye undergo ET and the other eye undergo CM, with treatment only if ROP progressed to threshold severity. For asymmetric cases (n = 84), the high-risk prethreshold eye was randomized to ET or CM.
Main outcome measure: Grating visual acuity measured at 6 years of age by masked testers using Teller acuity cards.
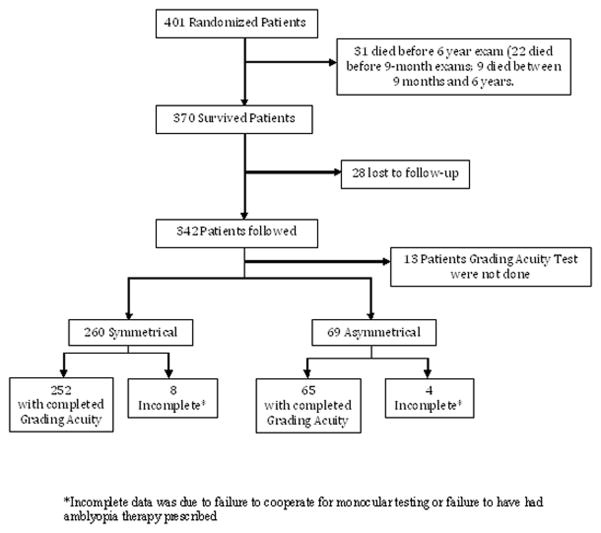
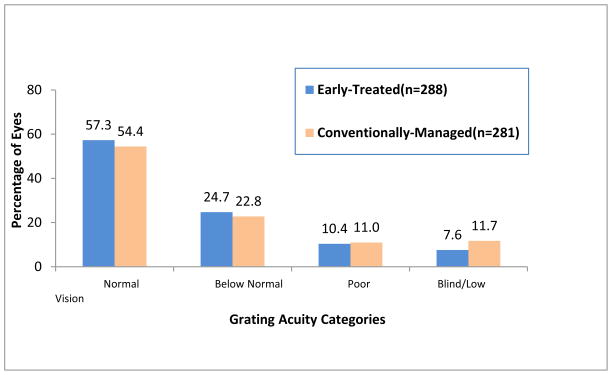
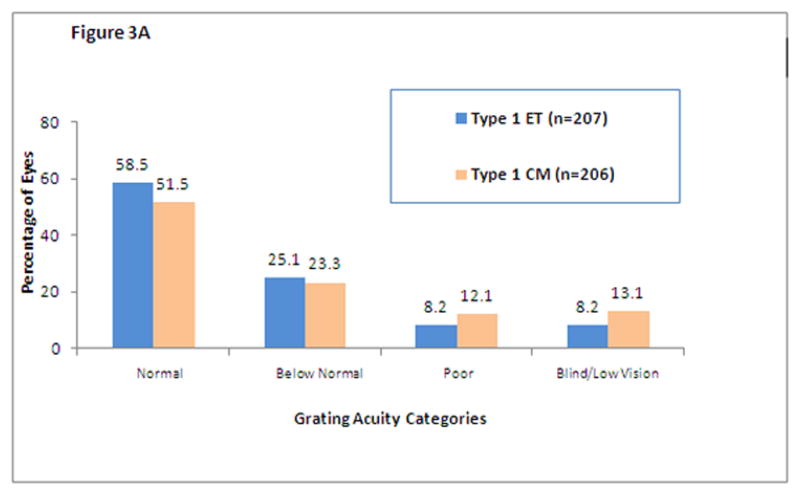
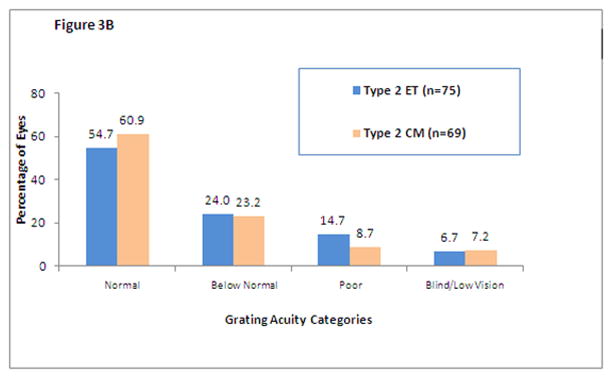
Results: Monocular grating acuity results were obtained from 317 of 370 surviving children (85.6%). Analysis of grating acuity results for all study participants with high-risk prethreshold ROP showed no statistically significant overall benefit of ET (18.1% vs 22.8% unfavorable outcomes; P = .08). When the 6-year grating acuity results were analyzed according to a clinical algorithm (high-risk types 1 and 2 prethreshold ROP), a benefit was seen in type 1 eyes (16.4% vs 25.2%; P = .004) undergoing ET, but not in type 2 eyes (21.3% vs 15.9%; P = .29).
Conclusion: Early treatment of eyes with type 1 ROP improves grating acuity outcomes, but ET for eyes with type 2 ROP does not. APPLICATION TO CLINICAL MEDICINE: Type 1 eyes should be treated early; however, based on acuity results at 6 years of age, type 2 eyes should be cautiously monitored for progression to type 1 ROP. Trial Registration clinicaltrials.gov Identifier: NCT00027222.
Conflict of interest statement
The authors have no affiliation with or financial interest in the subject matter or materials discussed in the paper (e.g., employment, consultancies, stock ownership, honoraria), with the exception of Velma Dobson, PhD, who has received royalties from the sale of Teller acuity cards.
Figures
References
-
- Hardy RJ, Palmer EA, Dobson V, Summers CG, Phelps DL, Quinn GE, Good WV, Tung B. Risk analysis of prethreshold retinopathy of prematurity. Arch Ophthalmol. 2003 Dec;121(12):1697–701. - PubMed
-
- Ferris FL, 3rd, Kassoff A, Bresnick GH, Bailey I. New visual acuity charts for clinical research. Am J Ophthalmol. 1982 Jul;94(1):91–6. - PubMed
-
- Teller DY, McDonald MA, Preston K, Sebris SL, Dobson V. Assessment of visual acuity in infants and children: the acuity card procedure. Dev Med Child Neurol. 1986 Dec;28(6):779–89. - PubMed
-
- Dobson V, Quinn GE, Biglan AW, Tung B, Flynn JT, Palmer EA. Acuity card assessment of visual function in the cryotherapy for retinopathy of prematurity trial. Invest Ophthalmol Vis Sci. 1990 Sep;31(9):1702–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
