

Iron overload decreases CaV1.3-dependent L-type Ca2+ currents leading to bradycardia, altered electrical conduction, and atrial fibrillation
- PMID: 21747058
- PMCID: PMC3401539
- DOI: 10.1161/CIRCEP.110.960401
Iron overload decreases CaV1.3-dependent L-type Ca2+ currents leading to bradycardia, altered electrical conduction, and atrial fibrillation
Abstract
Background: Chronic iron overload (CIO) is associated with blood disorders such as thalassemias and hemochromatosis. A major prognostic indicator of survival in patients with CIO is iron-mediated cardiomyopathy characterized by contractile dysfunction and electrical disturbances, including slow heart rate (bradycardia) and heart block.
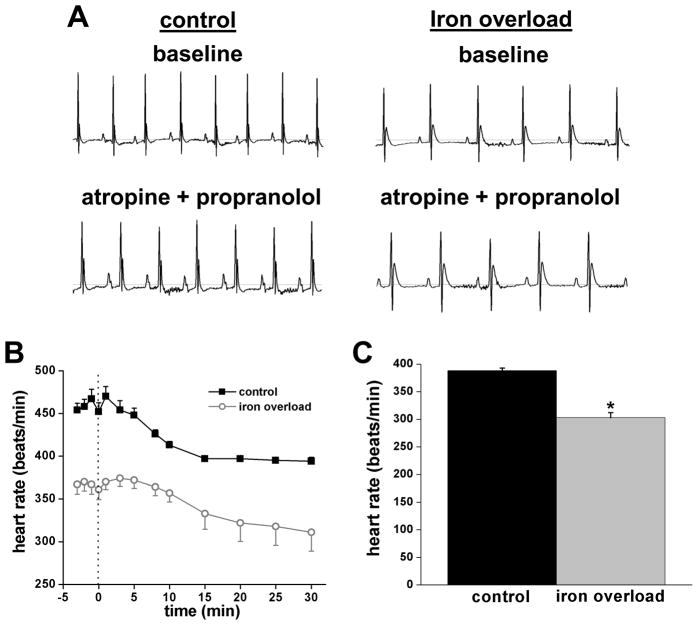
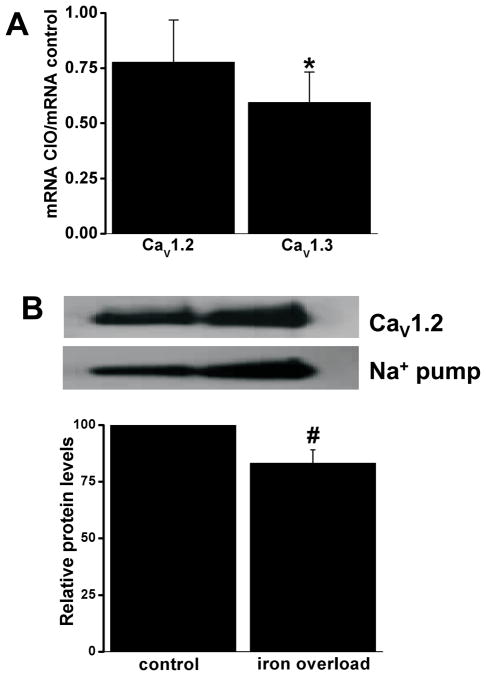
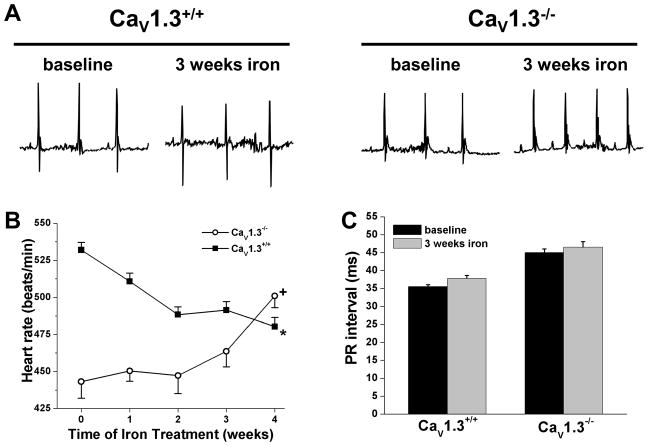
Methods and results: We used a mouse model of CIO to investigate the effects of iron on sinoatrial node (SAN) function. As in humans, CIO reduced heart rate (≈20%) in conscious mice as well as in anesthetized mice with autonomic nervous system blockade and in isolated Langendorff-perfused mouse hearts, suggesting that bradycardia originates from altered intrinsic SAN pacemaker function. Indeed, spontaneous action potential frequencies in SAN myocytes with CIO were reduced in association with decreased L-type Ca(2+) current (I(Ca,L)) densities and positive (rightward) voltage shifts in I(Ca,L) activation. Pacemaker current (I(f)) was not affected by CIO. Because I(Ca,L) in SAN myocytes (as well as in atrial and conducting system myocytes) activates at relatively negative potentials due to the presence of Ca(V)1.3 channels (in addition to Ca(V)1.2 channels), our data suggest that elevated iron preferentially suppresses Ca(V)1.3 channel function. Consistent with this suggestion, CIO reduced Ca(V)1.3 mRNA levels by ≈40% in atrial tissue (containing SAN) and did not lower heart rate in Ca(V)1.3 knockout mice. CIO also induced PR-interval prolongation, heart block, and atrial fibrillation, conditions also seen in Ca(V)1.3 knockout mice.
Conclusions: Our results demonstrate that CIO selectively reduces Ca(V)1.3-mediated I(Ca,L), leading to bradycardia, slowing of electrical conduction, and atrial fibrillation as seen in patients with iron overload.
Figures





Similar articles
-
Upregulation of adenosine A1 receptors facilitates sinoatrial node dysfunction in chronic canine heart failure by exacerbating nodal conduction abnormalities revealed by novel dual-sided intramural optical mapping.Circulation. 2014 Jul 22;130(4):315-24. doi: 10.1161/CIRCULATIONAHA.113.007086. Epub 2014 May 16. Circulation. 2014. PMID: 24838362 Free PMC article.
-
Distinct localization and modulation of Cav1.2 and Cav1.3 L-type Ca2+ channels in mouse sinoatrial node.J Physiol. 2012 Dec 15;590(24):6327-42. doi: 10.1113/jphysiol.2012.239954. Epub 2012 Oct 8. J Physiol. 2012. PMID: 23045342 Free PMC article.
-
Contribution of small conductance K+ channels to sinoatrial node pacemaker activity: insights from atrial-specific Na+ /Ca2+ exchange knockout mice.J Physiol. 2017 Jun 15;595(12):3847-3865. doi: 10.1113/JP274249. Epub 2017 May 13. J Physiol. 2017. PMID: 28346695 Free PMC article.
-
The role of the calcium and the voltage clocks in sinoatrial node dysfunction.Yonsei Med J. 2011 Mar;52(2):211-9. doi: 10.3349/ymj.2011.52.2.211. Yonsei Med J. 2011. PMID: 21319337 Free PMC article. Review.
-
T-type channels in the sino-atrial and atrioventricular pacemaker mechanism.Pflugers Arch. 2014 Apr;466(4):791-9. doi: 10.1007/s00424-014-1482-6. Epub 2014 Feb 27. Pflugers Arch. 2014. PMID: 24573175 Review.
Cited by
-
The Role of Ferroptosis in Atrial Fibrillation: A Promising Future.Rev Cardiovasc Med. 2024 Apr 1;25(4):127. doi: 10.31083/j.rcm2504127. eCollection 2024 Apr. Rev Cardiovasc Med. 2024. PMID: 39076535 Free PMC article. Review.
-
Functional role of voltage gated Ca(2+) channels in heart automaticity.Front Physiol. 2015 Feb 2;6:19. doi: 10.3389/fphys.2015.00019. eCollection 2015. Front Physiol. 2015. PMID: 25698974 Free PMC article. Review.
-
Deficiency of mitochondrial calcium uniporter abrogates iron overload-induced cardiac dysfunction by reducing ferroptosis.Basic Res Cardiol. 2023 May 25;118(1):21. doi: 10.1007/s00395-023-00990-7. Basic Res Cardiol. 2023. PMID: 37227592 Free PMC article.
-
Impact of Iron and Homocysteine Levels on T Peak-to-End Interval and Tp-e/QT Ratio in Elite Athletes.Ann Noninvasive Electrocardiol. 2016 Nov;21(6):557-565. doi: 10.1111/anec.12365. Epub 2016 Mar 28. Ann Noninvasive Electrocardiol. 2016. PMID: 27019094 Free PMC article.
-
Cardiac injury caused by iron overload in thalassemia.Front Pediatr. 2025 Jan 27;13:1514722. doi: 10.3389/fped.2025.1514722. eCollection 2025. Front Pediatr. 2025. PMID: 39931654 Free PMC article. Review.
References
-
- Buja LM, Roberts WC. Iron in the heart. Etiology and clinical significance. Am J Med. 1971;51:209–221. - PubMed
-
- Engle MA, Erlandson M, Smith CH. Late cardiac complications of chronic, severe, refractory anemia with hemochromatosis. Circulation. 1964;30:698–705. - PubMed
-
- Liu P, Olivieri N. Iron overload cardiomyopathies: new insights into an old disease. Cardiovasc Drugs Ther. 1994;8:101–110. - PubMed
-
- Aessopos A, Farmakis D, Karagiorga M, Voskaridou E, Loutradi A, Hatziliami A, Joussef J, Rombos J, Loukopoulos D. Cardiac involvement in thalassemia intermedia: a multicenter study. Blood. 2001;97:3411–3416. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
