

Encephalitis and antibodies to synaptic and neuronal cell surface proteins
- PMID: 21747075
- PMCID: PMC3140073
- DOI: 10.1212/WNL.0b013e318224afde
Encephalitis and antibodies to synaptic and neuronal cell surface proteins
Abstract
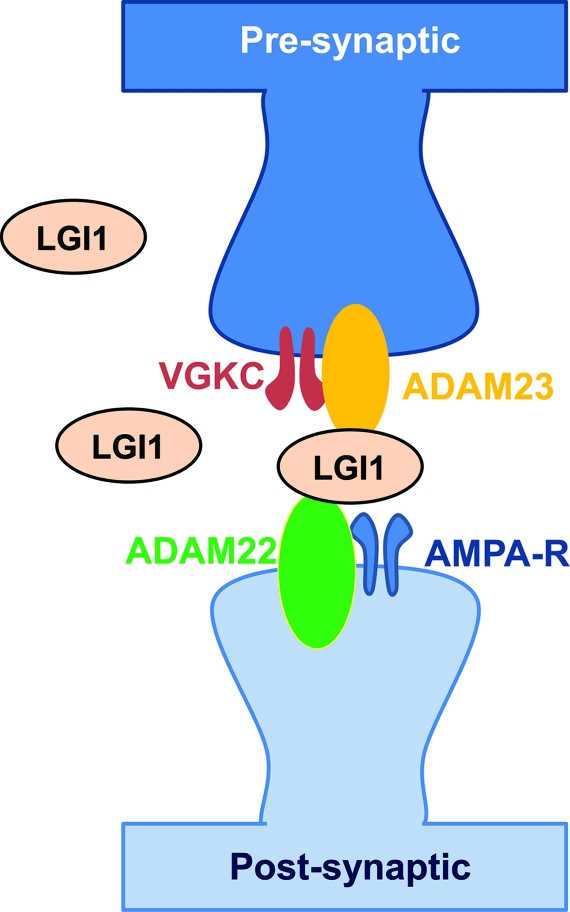
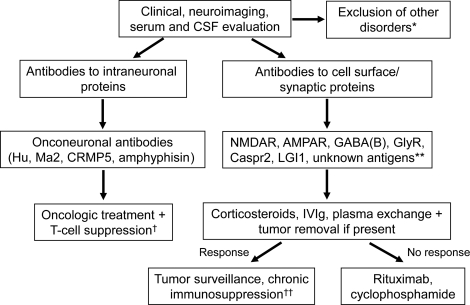
The identification of encephalitis associated with antibodies against cell surface and synaptic proteins, although recent, has already had a substantial impact in clinical neurology and neuroscience. The target antigens are receptors and proteins that have critical roles in synaptic transmission and plasticity, including the NMDA receptor, the AMPA receptor, the GABA(B) receptor, and the glycine receptor. Other autoantigens, such as leucine-rich glioma-inactivated 1 and contactin-associated protein-like 2, form part of trans-synaptic complexes and neuronal cell adhesion molecules involved in fine-tuning synaptic transmission and nerve excitability. Syndromes resulting from these immune responses resemble those of pharmacologic or genetic models in which the antigens are disrupted. For some immune responses, there is evidence that the antibodies alter the structure and function of the antigen, suggesting a direct pathogenic effect. These disorders are important because they can affect children and young adults, are severe and protracted, occur with or without tumor association, and respond to treatment but may relapse. This review provides an update on these syndromes and autoantigens with special emphasis on clinical diagnosis and treatment.
Figures
References
-
- Hutchinson M, Waters P, McHugh J, et al. Progressive encephalomyelitis, rigidity, and myoclonus: a novel glycine receptor antibody. Neurology 2008;71:1291–1292 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical