

Microsatellite instability and loss of heterozygosity at chromosomal location 18q: prospective evaluation of biomarkers for stages II and III colon cancer--a study of CALGB 9581 and 89803
- PMID: 21747089
- PMCID: PMC3157981
- DOI: 10.1200/JCO.2010.33.0092
Microsatellite instability and loss of heterozygosity at chromosomal location 18q: prospective evaluation of biomarkers for stages II and III colon cancer--a study of CALGB 9581 and 89803
Abstract
Purpose: Colorectal cancer (CRC) develops as a result of a series of accumulated genomic changes that produce oncogene activation and tumor suppressor gene loss. These characteristics may classify CRC into subsets of distinct clinical behaviors.
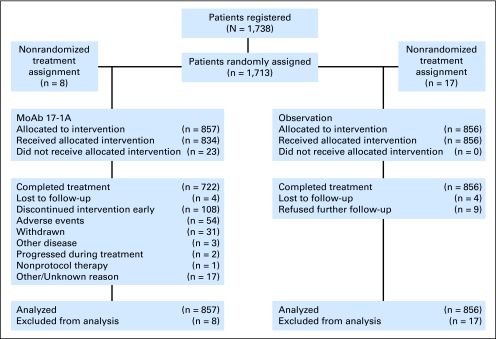
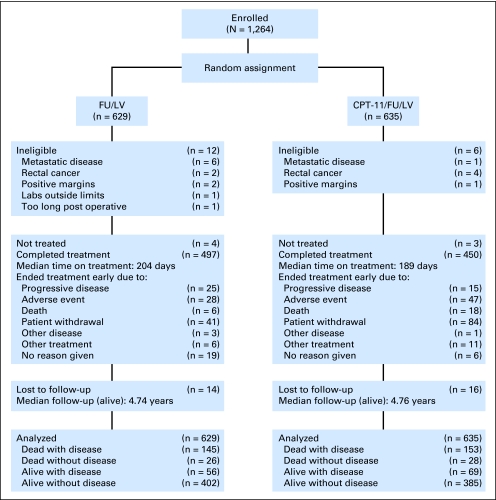
Patients and methods: We studied two of these genomic defects-mismatch repair deficiency (MMR-D) and loss of heterozygosity at chromosomal location 18q (18qLOH)-in patients enrolled onto two phase III cooperative group trials for treatment of potentially curable colon cancer. These trials included prospective secondary analyses to determine the relationship between these markers and treatment outcome. A total of 1,852 patients were tested for MMR status and 955 (excluding patients with MMR-D tumors) for 18qLOH.
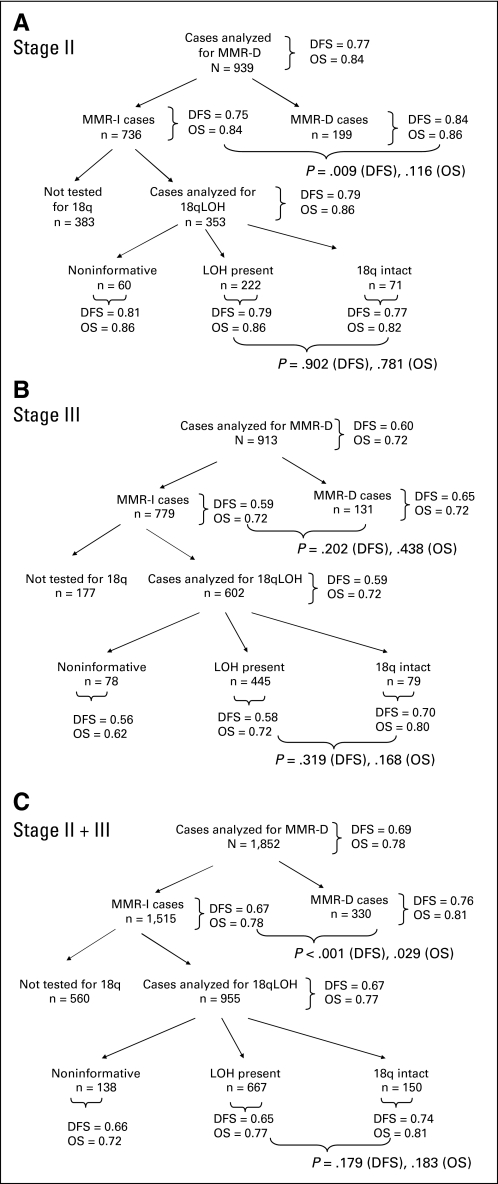
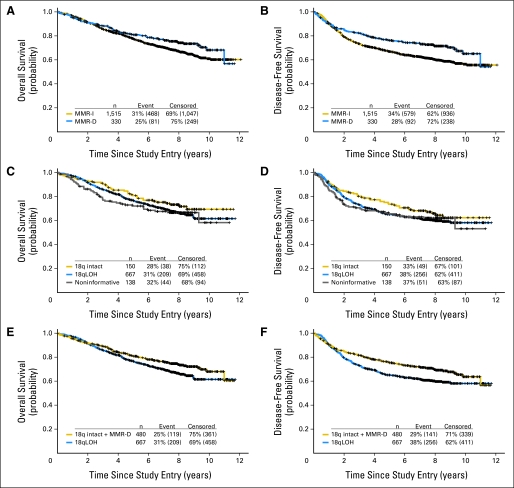
Results: Compared with stage III, more stage II tumors were MMR-D (21.3% v 14.4%; P < .001) and were intact at 18q (24.2% v 15.1%; P = .001). For the combined cohort, patients with MMR-D tumors had better 5-year disease-free survival (DFS; 0.76 v 0.67; P < .001) and overall survival (OS; 0.81 v 0.78; P = .029) than those with MMR intact (MMR-I) tumors. Among patients with MMR-I tumors, the status of 18q did not affect outcome, with 5-year values for patients with 18q intact versus 18qLOH tumors of 0.74 versus 0.65 (P = .18) for DFS and 0.81 versus 0.77 (P = .18) for OS.
Conclusion: We conclude that MMR-D tumor status, but not the presence of 18qLOH, has prognostic value for stages II and III colon cancer.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532. - PubMed
-
- Thibodeau S, Bren G, Schaid D. Microsatellite instability in cancer of the proximal colon. Science. 1993;260:616–619. - PubMed
-
- Samowitz WS, Curtin K, Ma KN, et al. Microsatellite instability in sporadic colon cancer is associated with an improved prognosis at the population level. Cancer Epidemiol Biomarkers Prev. 2001;10:917–932. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA077658/CA/NCI NIH HHS/United States
- U10 CA077597/CA/NCI NIH HHS/United States
- U10 CA114558/CA/NCI NIH HHS/United States
- U10 CA045418/CA/NCI NIH HHS/United States
- U10 CA041287/CA/NCI NIH HHS/United States
- U10 CA032102/CA/NCI NIH HHS/United States
- U10 CA021661/CA/NCI NIH HHS/United States
- U10 CA074811/CA/NCI NIH HHS/United States
- P30 CA016359/CA/NCI NIH HHS/United States
- U10 CA047577/CA/NCI NIH HHS/United States
- U10 CA032291/CA/NCI NIH HHS/United States
- CA33601/CA/NCI NIH HHS/United States
- U10 CA035091/CA/NCI NIH HHS/United States
- U10 CA052784/CA/NCI NIH HHS/United States
- U10 CA071323/CA/NCI NIH HHS/United States
- U10 CA086726/CA/NCI NIH HHS/United States
- N01 CA032102/CA/NCI NIH HHS/United States
- U10 CA045564/CA/NCI NIH HHS/United States
- U10 CA035279/CA/NCI NIH HHS/United States
- U10 CA077202/CA/NCI NIH HHS/United States
- U10 CA045808/CA/NCI NIH HHS/United States
- U10 CA012027/CA/NCI NIH HHS/United States
- U10 CA031946/CA/NCI NIH HHS/United States
- U10 CA021115/CA/NCI NIH HHS/United States
- U10 CA007968/CA/NCI NIH HHS/United States
- U10 CA033601/CA/NCI NIH HHS/United States
- U10 CA045389/CA/NCI NIH HHS/United States
- U10 CA021060/CA/NCI NIH HHS/United States
- U10 CA059518/CA/NCI NIH HHS/United States
- U10 CA035421/CA/NCI NIH HHS/United States
- U10 CA077440/CA/NCI NIH HHS/United States
- U10 CA037447/CA/NCI NIH HHS/United States
- U10 CA035113/CA/NCI NIH HHS/United States
- U10 CA047559/CA/NCI NIH HHS/United States
- U10 CA077651/CA/NCI NIH HHS/United States
- U10 CA025224/CA/NCI NIH HHS/United States
- U10 CA047642/CA/NCI NIH HHS/United States
- CA31946/CA/NCI NIH HHS/United States
- U10 CA003927/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
