

Prentice Award Lecture 2010: A case for peripheral optical treatment strategies for myopia
- PMID: 21747306
- PMCID: PMC3371664
- DOI: 10.1097/OPX.0b013e3182279cfa
Prentice Award Lecture 2010: A case for peripheral optical treatment strategies for myopia
Abstract
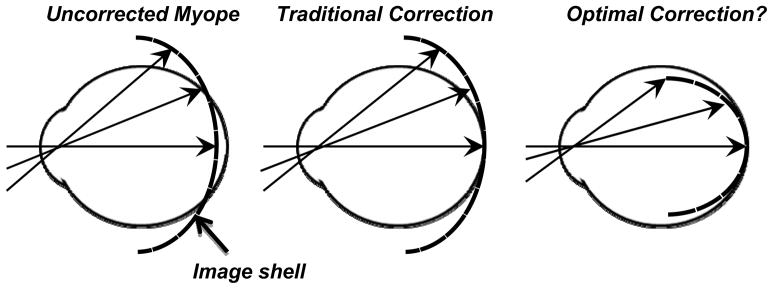
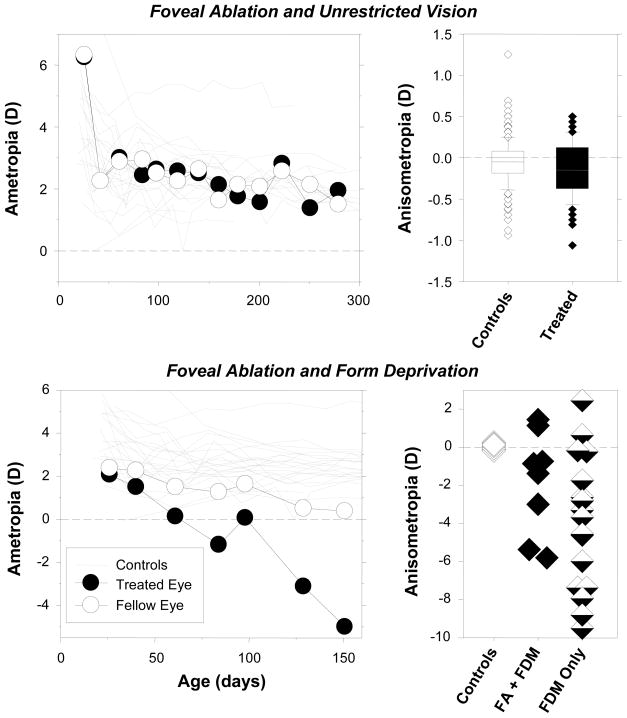
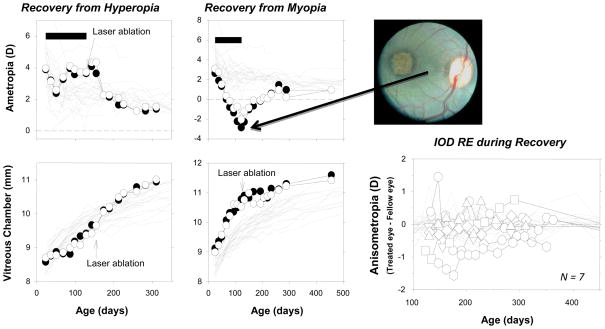
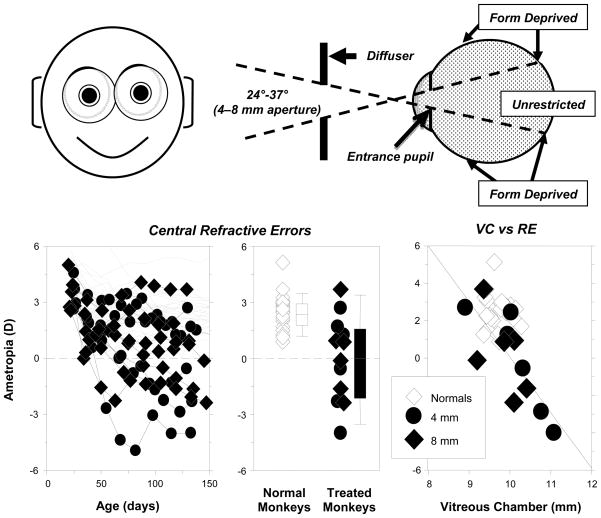
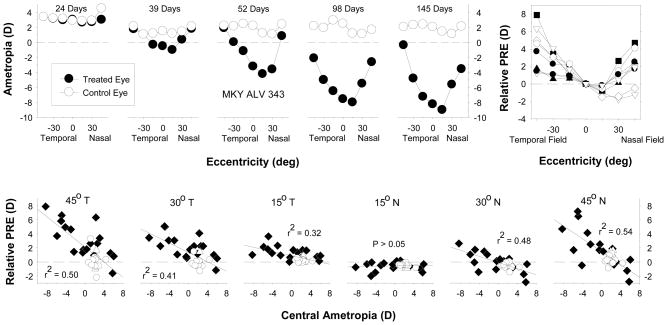
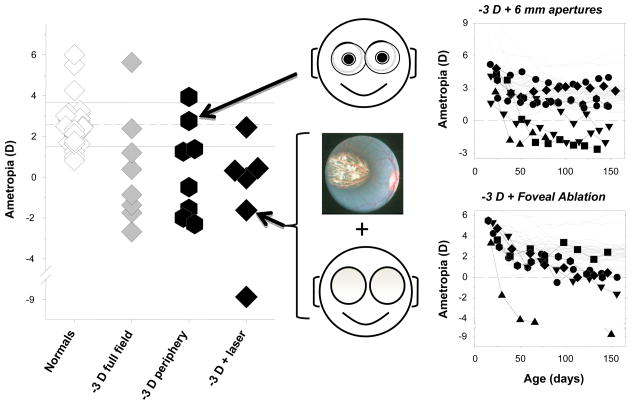
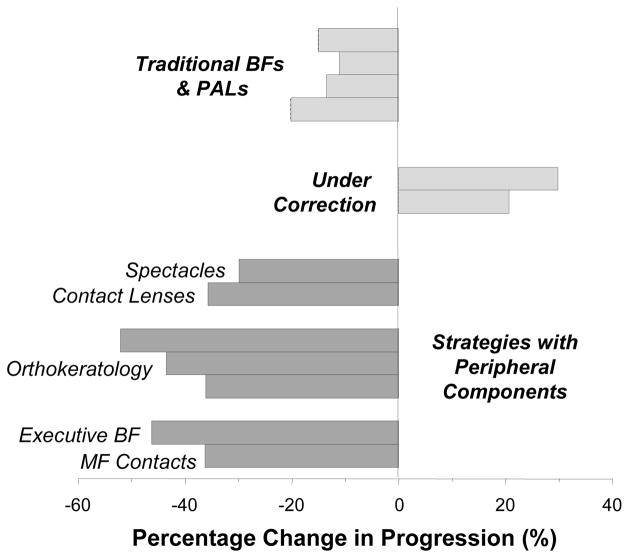
It is well established that refractive development is regulated by visual feedback. However, most optical treatment strategies designed to reduce myopia progression have not produced the desired results, primarily because some of our assumptions concerning the operating characteristics of the vision-dependent mechanisms that regulate refractive development have been incorrect. In particular, because of the prominence of central vision in primates, it has generally been assumed that signals from the fovea determine the effects of vision on refractive development. However, experiments in laboratory animals demonstrate that ocular growth and emmetropization are mediated by local retinal mechanisms and that foveal vision is not essential for many vision-dependent aspects of refractive development. However, the peripheral retina, in isolation, can effectively regulate emmetropization and mediate many of the effects of vision on the eye's refractive status. Moreover, when there are conflicting visual signals between the fovea and the periphery, peripheral vision can dominate refractive development. The overall pattern of results suggests that optical treatment strategies for myopia that take into account the effects of peripheral vision are likely to be more successful than strategies that effectively manipulate only central vision.
Figures
Similar articles
-
Effects of foveal ablation on emmetropization and form-deprivation myopia.Invest Ophthalmol Vis Sci. 2007 Sep;48(9):3914-22. doi: 10.1167/iovs.06-1264. Invest Ophthalmol Vis Sci. 2007. PMID: 17724167 Free PMC article.
-
Optical treatment strategies to slow myopia progression: effects of the visual extent of the optical treatment zone.Exp Eye Res. 2013 Sep;114:77-88. doi: 10.1016/j.exer.2012.11.019. Epub 2013 Jan 3. Exp Eye Res. 2013. PMID: 23290590 Free PMC article. Review.
-
Effects of foveal ablation on the pattern of peripheral refractive errors in normal and form-deprived infant rhesus monkeys (Macaca mulatta).Invest Ophthalmol Vis Sci. 2011 Aug 16;52(9):6428-34. doi: 10.1167/iovs.10-6757. Invest Ophthalmol Vis Sci. 2011. PMID: 21693598 Free PMC article.
-
Visual regulation of refractive development: insights from animal studies.Eye (Lond). 2014 Feb;28(2):180-8. doi: 10.1038/eye.2013.277. Epub 2013 Dec 13. Eye (Lond). 2014. PMID: 24336296 Free PMC article. Review.
-
Axial eye growth and refractive error development can be modified by exposing the peripheral retina to relative myopic or hyperopic defocus.Invest Ophthalmol Vis Sci. 2014 Sep 4;55(10):6765-73. doi: 10.1167/iovs.14-14524. Invest Ophthalmol Vis Sci. 2014. PMID: 25190657 Free PMC article.
Cited by
-
Update and guidance on management of myopia. European Society of Ophthalmology in cooperation with International Myopia Institute.Eur J Ophthalmol. 2021 May;31(3):853-883. doi: 10.1177/1120672121998960. Epub 2021 Mar 5. Eur J Ophthalmol. 2021. PMID: 33673740 Free PMC article.
-
Comparing the relative peripheral refraction effect of single vision and multifocal contact lenses measured using an autorefractor and an aberrometer: A pilot study.J Optom. 2015 Jul-Sep;8(3):206-18. doi: 10.1016/j.optom.2015.01.005. Epub 2015 Feb 7. J Optom. 2015. PMID: 25662364 Free PMC article.
-
Myopia Control with a Novel Peripheral Gradient Soft Lens and Orthokeratology: A 2-Year Clinical Trial.Biomed Res Int. 2015;2015:507572. doi: 10.1155/2015/507572. Epub 2015 Oct 28. Biomed Res Int. 2015. PMID: 26605331 Free PMC article. Clinical Trial.
-
Peripheral Retinal Vascular Patterns in Patients with Rhegmatogenous Retinal Detachment in Taiwan.PLoS One. 2016 Feb 24;11(2):e0149176. doi: 10.1371/journal.pone.0149176. eCollection 2016. PLoS One. 2016. PMID: 26909812 Free PMC article. Clinical Trial.
-
Development and evaluation of machine learning models for individualized prediction of myopia control efficacy treated with overnight orthokeratology.Front Med (Lausanne). 2025 May 12;12:1559435. doi: 10.3389/fmed.2025.1559435. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40421305 Free PMC article.
References
-
- Sperduto RD, Seigel D, Roberts J, Rowland M. Prevalence of myopia in the United States. Arch Ophthalmol. 1983;101:405–7. - PubMed
-
- Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33:27–33. - PubMed
-
- Hosaka A. Population studies—myopia experience in Japan. Acta Ophthalmol Suppl. 1988;185:37–40. - PubMed
-
- Woo WW, Lim KA, Yang H, Lim XY, Liew F, Lee YS, Saw SM. Refractive errors in medical students in Singapore. Singapore Med J. 2004;45:470–4. - PubMed
-
- Wu MM, Edwards MH. The effect of having myopic parents: an analysis of myopia in three generations. Optom Vis Sci. 1999;76:387–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
