

Treatment outcomes in children with Burkitt lymphoma and L3 acute lymphoblastic leukemia treated using the lymphoma malignancy B protocol at a single institution
- PMID: 21747881
- PMCID: PMC3128907
- DOI: 10.5045/kjh.2011.46.2.96
Treatment outcomes in children with Burkitt lymphoma and L3 acute lymphoblastic leukemia treated using the lymphoma malignancy B protocol at a single institution
Abstract
Background: We compared the outcomes of patients with Burkitt lymphoma and French-American-British (FAB) L3 acute lymphoblastic leukemia treated using Lymphoma Malignancy B (LMB) or other treatment protocols.
Methods: Thirty-eight patients diagnosed between July 1996 and December 2007 were treated using LMB 96, and 22 patients diagnosed between January 1991 and May 1998 (defined as the early period) were treated using the D-COMP or CCG-106B protocols. We retrospectively reviewed their medical records and analyzed cumulative survival according to the treatment period by using Kaplan-Meier analysis.
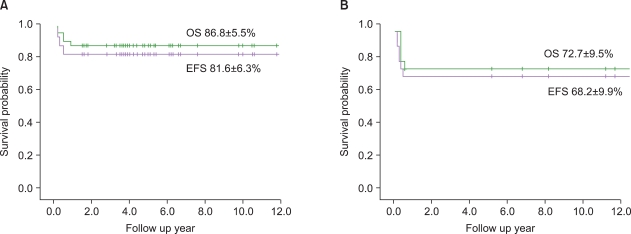
Results: There were no intergroup differences in the distribution of age, disease stage, or risk group. The median follow-up period of the 33 live patients in the LMB group was 72 months (range, 36-170 months). Overall survival (OS) and event-free survival (EFS) of patients treated using LMB 96 were 86.8%±5.5% and 81.6%±6.3%, respectively, whereas OS and EFS of patients treated in the early period were 72.7%±9.6% and 68.2%±9.9%, respectively. In the LMB 96 group, OS of cases showing non-complete response (N=8) was 62.5%±17.1%, and OS of relapsed or primary refractory cases (N=6) was 33.3%±19.3%. Central nervous system (CNS) disease, high lactate dehydrogenase levels at diagnosis, and treatment response were significant prognostic factors.
Conclusion: Survival outcome has drastically improved over the last 2 decades with short-term, dose-intensive chemotherapy. However, CNS involvement or poor response to chemotherapy was worse prognostic factors; therefore, future studies addressing this therapeutic challenge are warranted.
Keywords: Burkitt lymphoma; L3 lymphocytic leukemia; Prognosis; Treatment outcome.
Figures





References
-
- Sandlund JT, Downing JR, Crist WM. Non-Hodgkin's lymphoma in childhood. N Engl J Med. 1996;334:1238–1248. - PubMed
-
- Hecht JL, Aster JC. Molecular biology of Burkitt's lymphoma. J Clin Oncol. 2000;18:3707–3721. - PubMed
-
- Patte C, Philip T, Rodary C, et al. Improved survival rate in children with stage III and IV B cell non-Hodgkin's lymphoma and leukemia using multi-agent chemotherapy: results of a study of 114 children from the French Pediatric Oncology Society. J Clin Oncol. 1986;4:1219–1226. - PubMed
-
- Patte C, Philip T, Rodary C, et al. High survival rate in advanced-stage B-cell lymphomas and leukemias without CNS involvement with a short intensive polychemotherapy: results from the French Pediatric Oncology Society of a randomized trial of 216 children. J Clin Oncol. 1991;9:123–132. - PubMed
-
- Gentet JC, Patte C, Quintana E, et al. Phase II study of cytarabine and etoposide in children with refractory or relapsed non-Hodgkin's lymphoma: a study of the French Society of Pediatric Oncology. J Clin Oncol. 1990;8:661–665. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
