

Pupillary reactivity as an early indicator of increased intracranial pressure: The introduction of the Neurological Pupil index
- PMID: 21748035
- PMCID: PMC3130361
- DOI: 10.4103/2152-7806.82248
Pupillary reactivity as an early indicator of increased intracranial pressure: The introduction of the Neurological Pupil index
Abstract
Background: This paper introduces the 7/5/2011al Pupil index (NPi), a sensitive measure of pupil reactivity and an early indicator of increasing intracranial pressure (ICP). This may occur in patients with severe traumatic brain injury (TBI), aneurysmal subarachnoid hemorrhage, or intracerebral hemorrhage (ICH).
Methods: 134 patients (mean age 46 years, range 18-87 years, 54 women and 80 men) in the intensive care units at eight different clinical sites were enrolled in the study. Pupillary examination was performed using a portable hand-held pupillometer.
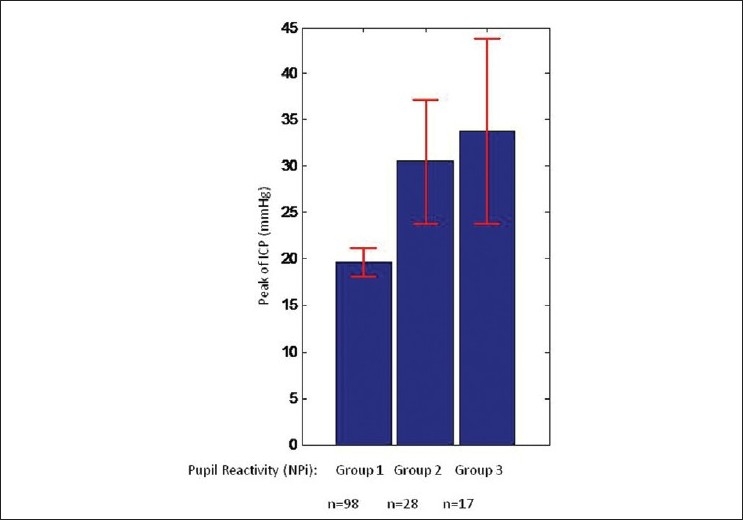
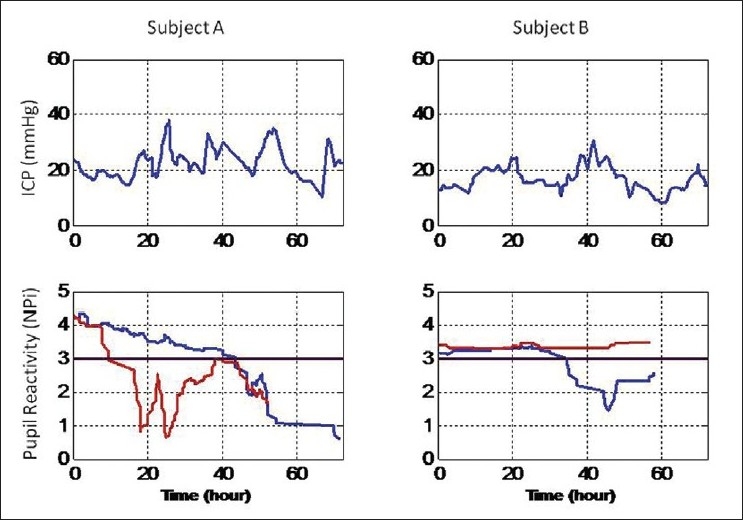
Results: Patients with abnormal pupillary light reactivity had an average peak ICP of 30.5 mmHg versus 19.6 mmHg for the normal pupil reactivity population (P = 0.0014). Patients with "nonreactive pupils" had the highest peaks of ICP (mean = 33.8 mmHg, P = 0.0046). In the group of patients with abnormal pupillary reactivity, we found that the first evidence of pupil abnormality occurred, on average, 15.9 hours prior to the time of the peak of ICP.
Conclusions: Automated pupillary assessment was used in patients with possible increased ICP. Using NPi, we were able to identify a trend of inverse relationship between decreasing pupil reactivity and increasing ICP. Quantitative measurement and classification of pupillary reactivity using NPi may be a useful tool in the early management of patients with causes of increased ICP.
Keywords: Intracranial pressure; Neurological Pupil index; pupillometer; traumatic brain injury.
Figures

References
-
- Andrews BT, Pitts LH. Functional recovery after traumatic transtentorial herniation. Neurosurgery. 1991;9:227–31. - PubMed
-
- Braakman R, Gelpke GJ, Habbema JD, Maas AI, Minderhoud JM. Systematic selection of prognostic features in patients with severe head injury. Neurosurgery. 1980;6:362–70. - PubMed
-
- Chesnut RM, Gautille T, Blunt BA, Klauber MR, Marshall LF. The localizing value of asymmetry in pupillary size in severe head injury: Relation to lesion type and location. Neurosurgery. 1994;34:840–6. - PubMed
-
- Chestnut RM, Ghajar J, Maas AI, Marion DW, Servadei F, Teasdale GM, et al. Management and prognosis of severe traumatic brain injury. New York: Brain Tumour Foundation, Inc; 2000. Early indicators of prognosis in severe traumatic brain injury.
-
- Chieregato A, Martino C, Pransani V, Nori G, Russo E, Noto A, et al. Classification of a traumatic brain injury: The Glasgow Coma scale is not enough. Acta Anaesthesiol Scand. 2010;54:696–702. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
