

Is the operative delivery rate in low-risk women dependent on the level of birth care? A randomised controlled trial
- PMID: 21749629
- PMCID: PMC3187863
- DOI: 10.1111/j.1471-0528.2011.03043.x
Is the operative delivery rate in low-risk women dependent on the level of birth care? A randomised controlled trial
Erratum in
- BJOG. 2011 Dec;118(13):1688
Abstract
Objective: To investigate possible differences in operative delivery rate among low-risk women, randomised to an alongside midwifery-led unit or to standard obstetric units within the same hospital.
Design: Randomised controlled trial.
Setting: Department of Obstetrics and Gynaecology, Østfold Hospital Trust, Tromsø, Norway.
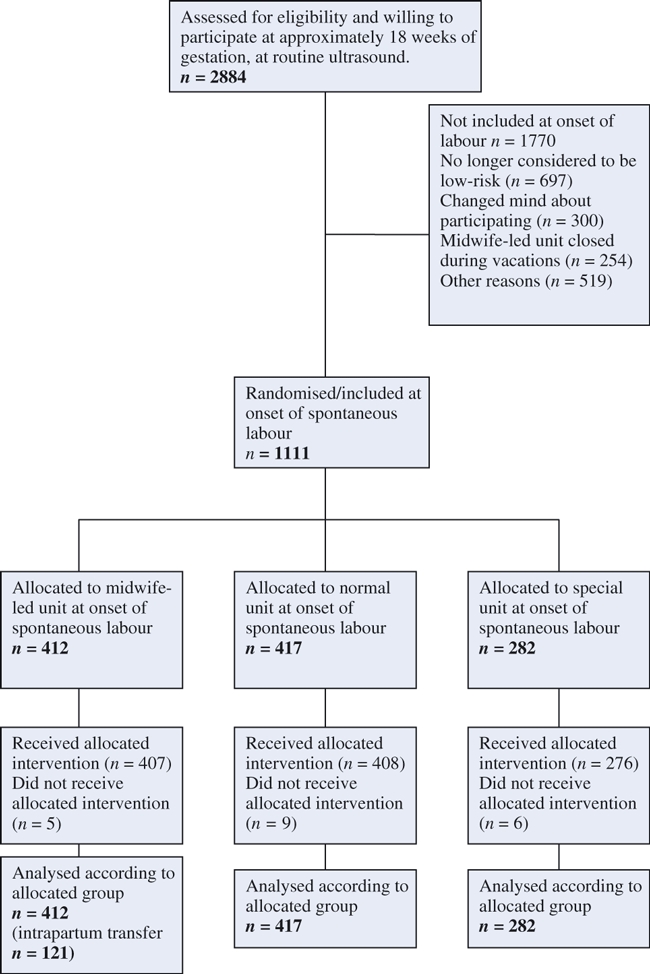
Population: A total of 1111 women assessed to be at low risk at onset of spontaneous labour.
Methods: Randomisation into one of three birth units: the special unit; the normal unit; or the midwife-led unit.
Main outcome measures: Total operative delivery rate, augmentation, pain relief, postpartum haemorrhage, sphincter injuries and intrapartum transfer, Apgar score <7 at 5 minutes, metabolic acidosis and transfer to neonatal intensive care unit.
Results: There were no significant differences in total operative deliveries between the three units: 16.3% in the midwife-led unit; 18.0% in the normal unit; and 18.8% in the special unit. There were no significant differences in postpartum haemorrhage, sphincter injuries or in neonatal outcomes. There were statistically significant differences in augmentation (midwife-led unit versus normal unit RR 0.73, 95% CI 0.59-0.89; midwife-led unit versus special unit RR 0.69, 95% CI 0.56-0.86), in epidural analgesia (midwife-led unit versus normal unit RR 0.68, 95% CI 0.52-0.90; midwife-led unit versus special unit RR 0.64, 95% CI 0.47-0.86) and in acupuncture (midwife-led unit versus normal unit RR 1.45, 95% CI 1.25-1.69; midwife-led unit versus special unit RR 1.45, 95% CI 1.22-1.73).
Conclusions: The level of birth care does not significantly affect the rate of operative deliveries in low-risk women without any expressed preference for level of birth care.
© 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology © 2011 RCOG.
Figures
Comment in
-
Level of birth care and operative delivery rates.BJOG. 2012 Feb;119(3):377; author reply 377-8. doi: 10.1111/j.1471-0528.2011.03208.x. BJOG. 2012. PMID: 22239420 No abstract available.
References
-
- Albers LL. Overtreatment of normal childbirth in U.S. hospitals. Birth. 2005;32:67–8. - PubMed
-
- Albers LL, Katz VL. Birth setting for low-risk pregnancies. An analysis of the current literature. J Nurse Midwifery. 1991;36:215–20. - PubMed
-
- Mead MM, Kornbrot D. The influence of maternity units’ intrapartum intervention rates and midwives’ risk perception for women suitable for midwifery-led care. Midwifery. 2004;20:61–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
