

Carfilzomib interacts synergistically with histone deacetylase inhibitors in mantle cell lymphoma cells in vitro and in vivo
- PMID: 21750224
- PMCID: PMC3170445
- DOI: 10.1158/1535-7163.MCT-10-1108
Carfilzomib interacts synergistically with histone deacetylase inhibitors in mantle cell lymphoma cells in vitro and in vivo
Retraction in
-
Retraction: Carfilzomib Interacts Synergistically with Histone Deacetylase Inhibitors in Mantle Cell Lymphoma Cells In Vitro and In Vivo.Mol Cancer Ther. 2019 Jun;18(6):1179. doi: 10.1158/1535-7163.MCT-19-0469. Mol Cancer Ther. 2019. PMID: 31160509 Free PMC article. No abstract available.
Abstract
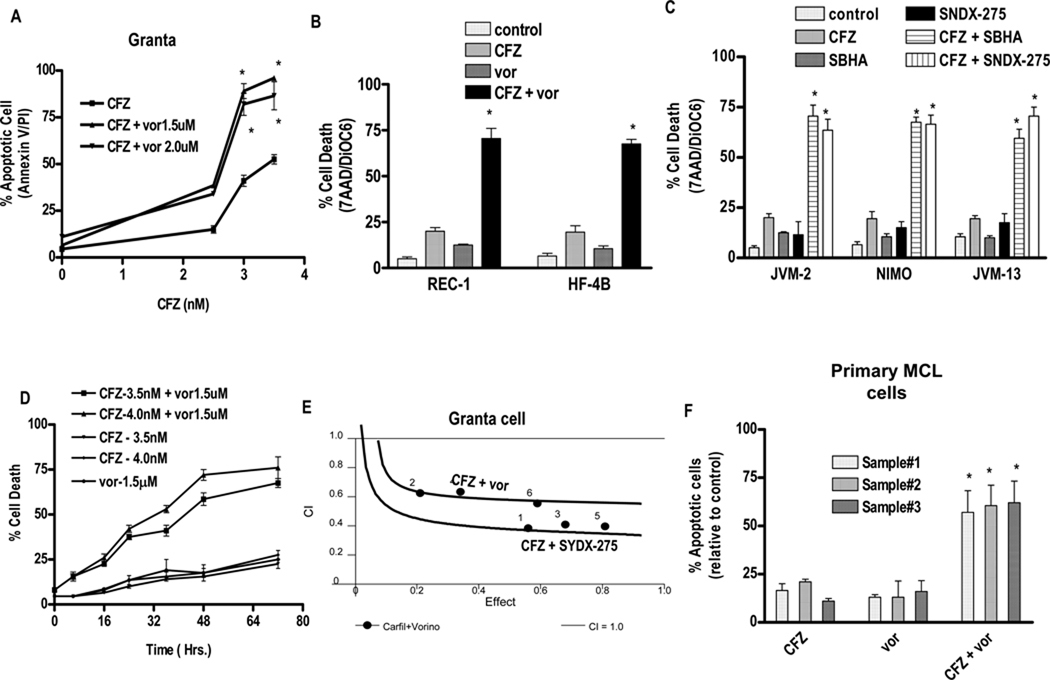
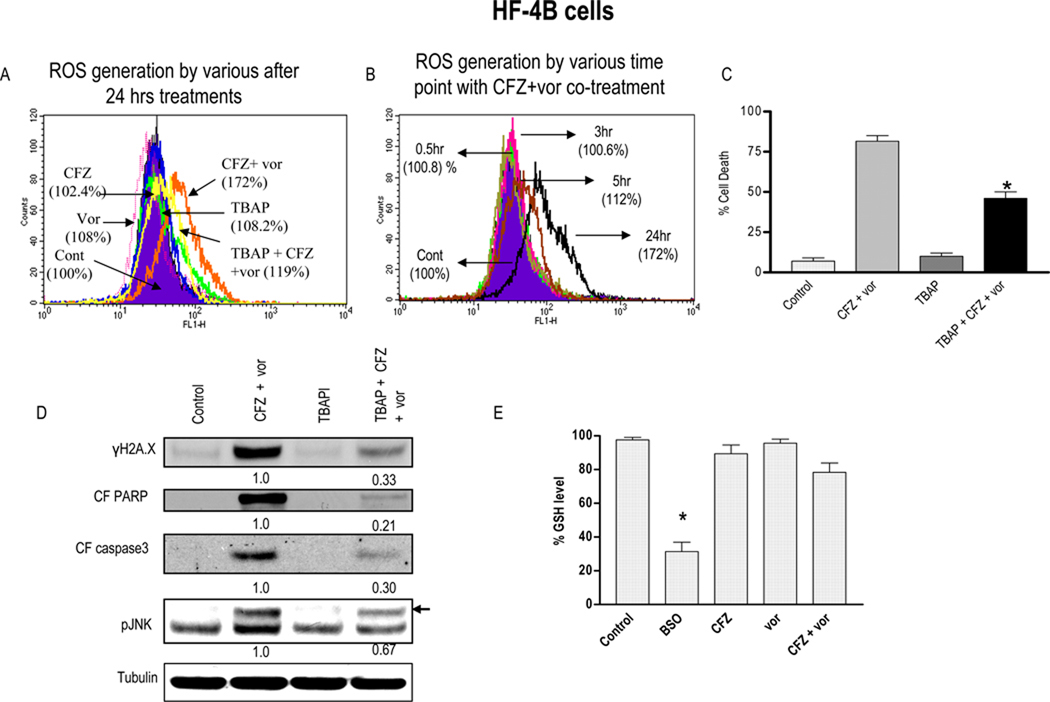
Interactions between the proteasome inhibitor carfilzomib and the histone deacetylase (HDAC) inhibitors vorinostat and SNDX-275 were examined in mantle cell lymphoma (MCL) cells in vitro and in vivo. Coadministration of very low, marginally toxic carfilzomib concentrations (e.g., 3-4 nmol/L) with minimally lethal vorinostat or SNDX-275 concentrations induced sharp increases in mitochondrial injury and apoptosis in multiple MCL cell lines and primary MCL cells. Enhanced lethality was associated with c-jun-NH,-kinase (JNK) 1/2 activation, increased DNA damage (induction of λH2A.X), and ERK1/2 and AKT1/2 inactivation. Coadministration of carfilzomib and histone deacetylase inhibitors (HDACI) induced a marked increase in reactive oxygen species (ROS) generation and G(2)-M arrest. Significantly, the free radical scavenger tetrakis(4-benzoic acid) porphyrin (TBAP) blocked carfilzomib/HDACI-mediated ROS generation, λH2A.X formation, JNK1/2 activation, and lethality. Genetic (short hairpin RNA) knockdown of JNK1/2 significantly attenuated carfilzomib/HDACI-induced apoptosis, but did not prevent ROS generation or DNA damage. Carfilzomib/HDACI regimens were also active against bortezomib-resistant MCL cells. Finally, carfilzomib/vorinostat coadministration resulted in a pronounced reduction in tumor growth compared with single agent treatment in an MCL xenograft model associated with enhanced apoptosis, λH2A.X formation, and JNK activation. Collectively, these findings suggest that carfilzomib/HDACI regimens warrant attention in MCL.
Conflict of interest statement
Potential conflict of interest: No conflict of interest to report
Figures




Comment in
-
Findings of Research Misconduct.NIH Guide Grants Contracts (Bethesda). 2015 Dec 18:NOT-OD-16-040. NIH Guide Grants Contracts (Bethesda). 2015. PMID: 26693581 Free PMC article. No abstract available.
-
Findings of Research Misconduct.Fed Regist. 2015 Dec 10;80(237):76703-76704. Fed Regist. 2015. PMID: 27737268 Free PMC article. No abstract available.
References
-
- Leonard JP, Williams ME, Goy A, Grant S, Pfreundschuh M, Rosen ST, et al. Mantle cell lymphoma: biological insights and treatment advances. Clin Lymphoma Myeloma. 2009;9:267–277. - PubMed
-
- Jares P, Colomer D, Campo E. Genetic and molecular pathogenesis of mantle cell lymphoma: perspectives for new targeted therapeutics. Nat Rev Cancer. 2007;7:750–762. - PubMed
-
- Schmidt C, Dreyling M. Therapy of mantle cell lymphoma: current standards and future strategies. Hematol Oncol Clin North Am. 2008;22:953–963. - PubMed
-
- Barr P, Fisher R, Friedberg J. The role of bortezomib in the treatment of lymphoma. Cancer Invest. 2007;25:766–775. - PubMed
-
- Cheson BD, Rummel MJ. Bendamustine: rebirth of an old drug. J Clin Oncol. 2009;27:1492–1501. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
