

Accuracy of five algorithms to diagnose gambiense human African trypanosomiasis
- PMID: 21750745
- PMCID: PMC3130008
- DOI: 10.1371/journal.pntd.0001233
Accuracy of five algorithms to diagnose gambiense human African trypanosomiasis
Abstract
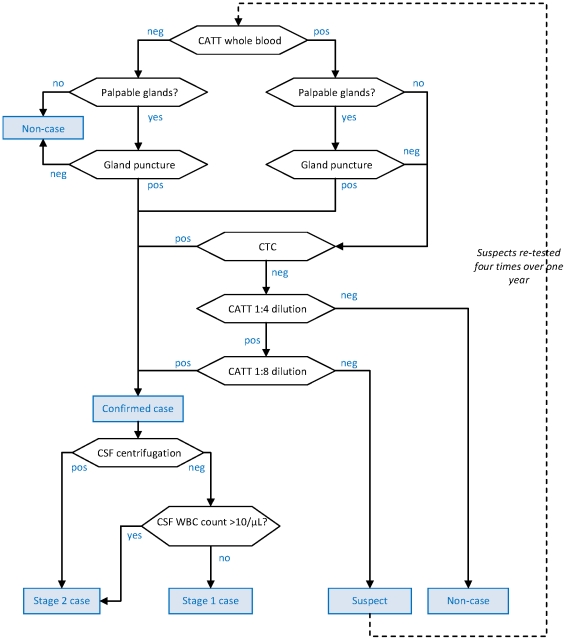
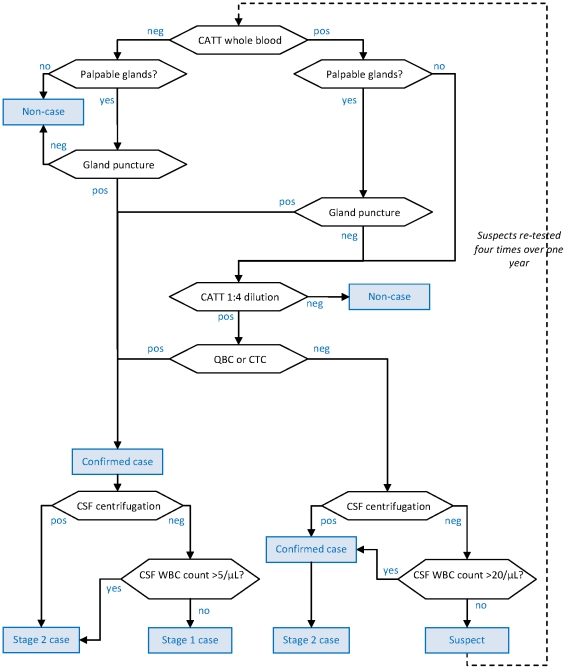
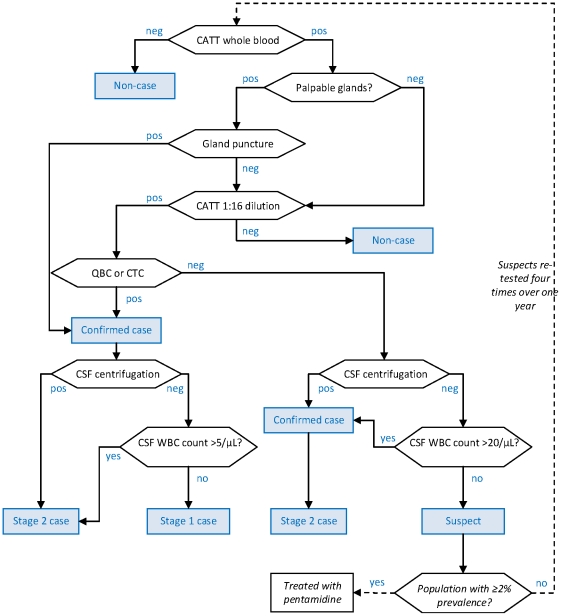
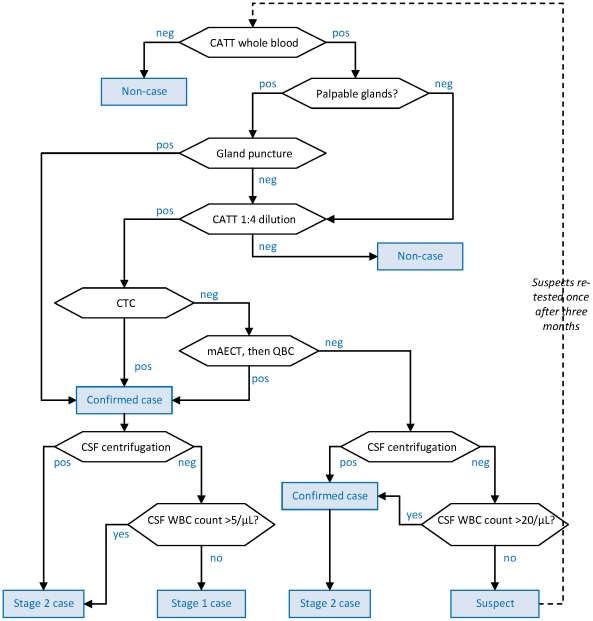
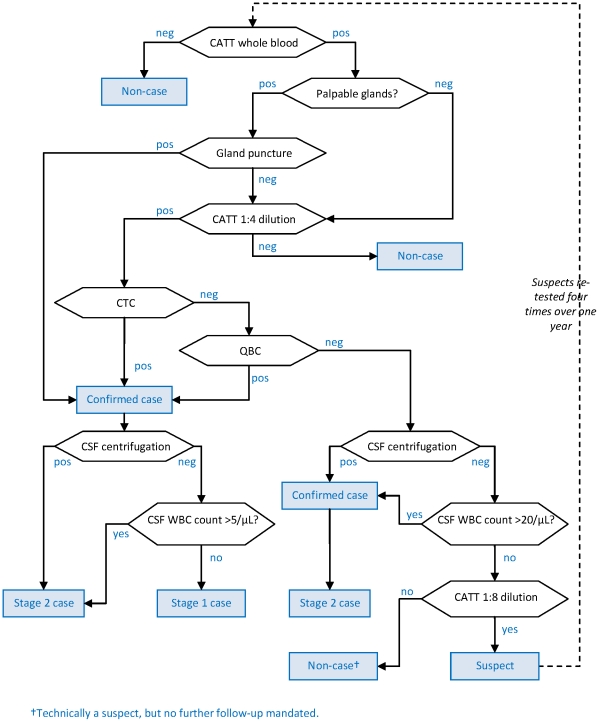
Background: Algorithms to diagnose gambiense human African trypanosomiasis (HAT, sleeping sickness) are often complex due to the unsatisfactory sensitivity and/or specificity of available tests, and typically include a screening (serological), confirmation (parasitological) and staging component. There is insufficient evidence on the relative accuracy of these algorithms. This paper presents estimates of the accuracy of five algorithms used by past Médecins Sans Frontières programmes in the Republic of Congo, Southern Sudan and Uganda.
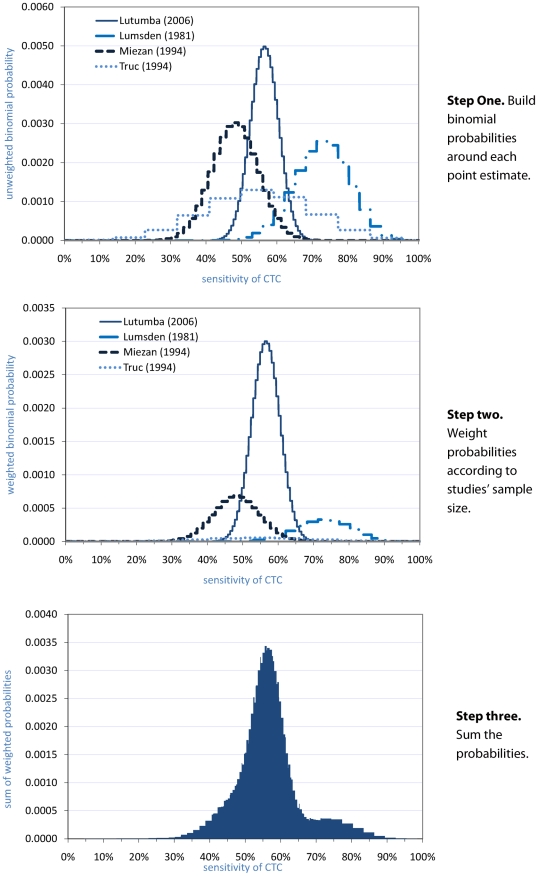
Methodology and principal findings: The sequence of tests in each algorithm was programmed into a probabilistic model, informed by distributions of the sensitivity, specificity and staging accuracy of each test, constructed based on a literature review. The accuracy of algorithms was estimated in a baseline scenario and in a worst-case scenario introducing various near worst-case assumptions. In the baseline scenario, sensitivity was estimated as 85-90% in all but one algorithm, with specificity above 99.9% except for the Republic of Congo, where CATT serology was used as independent confirmation test: here, positive predictive value (PPV) was estimated at <50% in realistic active screening prevalence scenarios. Furthermore, most algorithms misclassified about one third of true stage 1 cases as stage 2, and about 10% of true stage 2 cases as stage 1. In the worst-case scenario, sensitivity was 75-90% and PPV no more than 75% at 1% prevalence, with about half of stage 1 cases misclassified as stage 2.
Conclusions: Published evidence on the accuracy of widely used tests is scanty. Algorithms should carefully weigh the use of serology alone for confirmation, and could enhance sensitivity through serological suspect follow-up and repeat parasitology. Better evidence on the frequency of low-parasitaemia infections is needed. Simulation studies should guide the tailoring of algorithms to specific scenarios of HAT prevalence and availability of control tools.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Blum J, Nkunku S, Burri C. Clinical description of encephalopathic syndromes and risk factors for their occurrence and outcome during melarsoprol treatment of human African trypanosomiasis. Trop Med Int Health. 2001;6:390–400. - PubMed
-
- Magnus E, Vervoort T, Van Meirvenne N. A card-agglutination test with stained trypanosomes (C.A.T.T.) for the serological diagnosis of T. B. gambiense trypanosomiasis. Ann Soc Belg Med Trop. 1978;58:169–176. - PubMed
-
- Lejon V, Buscher P. Review Article: cerebrospinal fluid in human African trypanosomiasis: a key to diagnosis, therapeutic decision and post-treatment follow-up. Trop Med Int Health. 2005;10:395–403. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
